J Korean Orthop Assoc.
2013 Aug;48(4):314-318.
Correction of Congenital Metacarpal Synostosis with Polypropylene Mesh as an Interpositional Material
- Affiliations
-
- 1Department of Orthopedic Surgery, Hallym University Sacred Heart Hospital, Anyang, Korea. pedoskwak@hallym.or.kr
Abstract
- Metacarpal synostosis is an uncommon congenital hand malformation characterized by the coalescence of two or more adjacent metacarpals. Patients visit the hospital due to abduction deformity, which is usually a mild deformity or a minor functional deficit. This is one of the reasons why the patient goes to the hospital late and foregoes proper management with early detection and treatment. A number of surgical procedures ranging from simple to complex have been employed for treatment of this deformity. We describe our experience with a longitudinal osteotomy, realignment of component metacarpals with the metacarpophalangeal joint, and interposition of a non-absorbable polypropylene mesh used for inguinal hernia for correction of the abducted deformity and prevention of recurrence of synostosis while minimizing morbidity.
Keyword
MeSH Terms
Figure
-
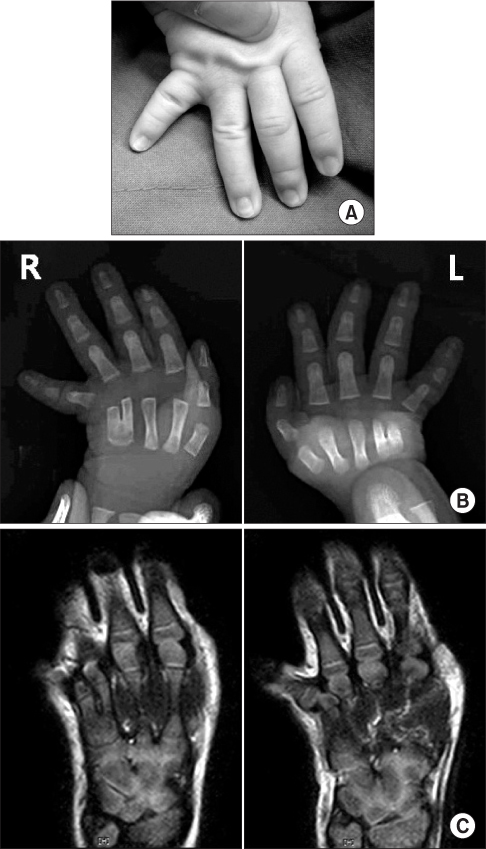
Figure 1 Preoperative evaluation. (A) Clinical photo of the hand shows marked abduction of the fifth finger. (B) Preoperative radiographs show bilateral metacarpal synostosis of the fourth and fifth fingers. (C) Preoperative magnetic resonance image shows a hypoplastic metacarphop haryngeal joint.
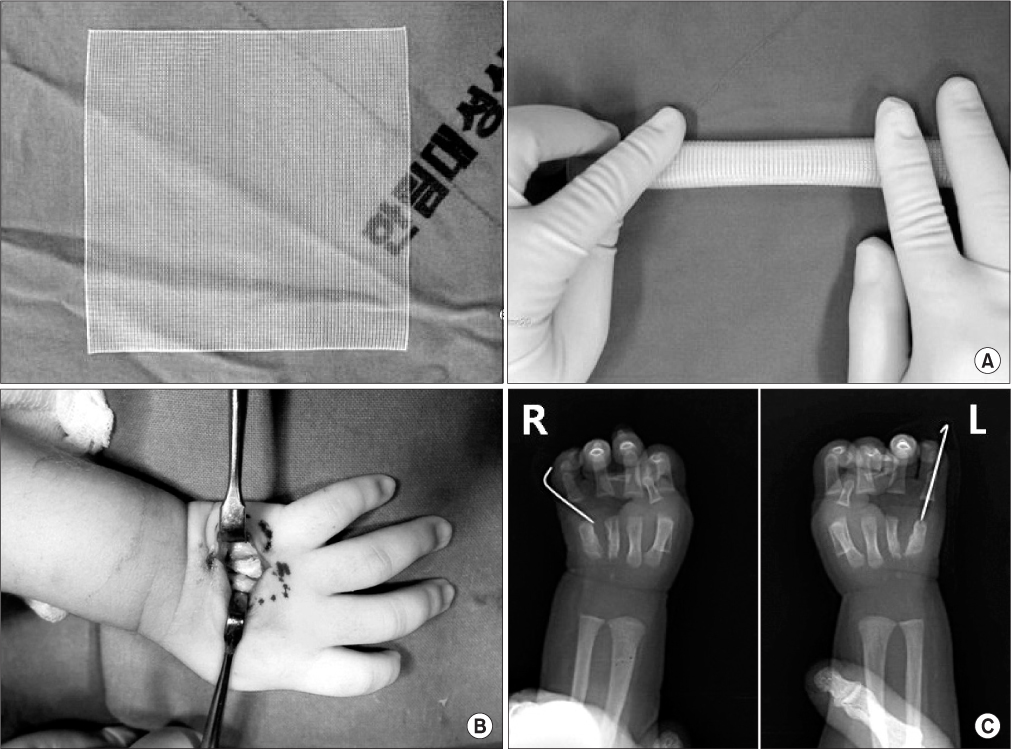
Figure 2 Surgical procedure. (A) Polypropylene mesh is crumpled into a roll. (B) Obvolutive mesh is inserted into the osteotomy site. (C) The mesh is held in place and a Kirschner's wire is fixed for stability of the joint.
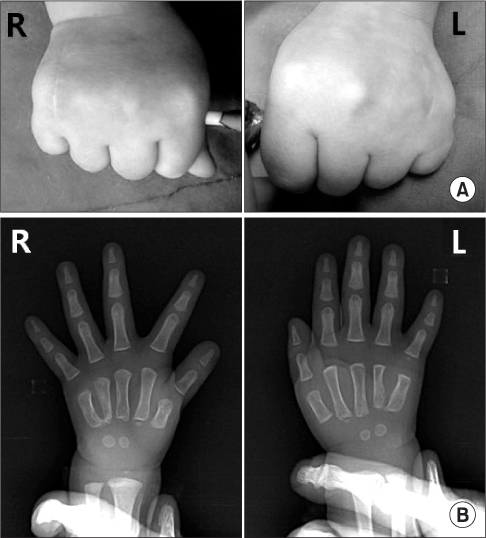
Figure 3 Postoperative evaluation. (A) Clinical photo of the patient at final follow-up shows functional improvement with corrected deformity. (B) Final radiographs show no recurrence.
Reference
-
1. Miura T. Congenital synostosis between the fourth and fifth metacarpal bones. J Hand Surg Am. 1988; 13:83–88.
Article2. Buck-Gramcko D, Wood VE. The treatment of metacarpal synostosis. J Hand Surg Am. 1993; 18:565–581.
Article3. Foucher G, Navarro R, Medina J, Khouri RK. Metacarpal synostosis: a simple classification and a new treatment technique. Plast Reconstr Surg. 2001; 108:1225–1231.
Article4. Kawabata H, Yasui N, Che YH, Hirooka A. Treatment for congenital synostosis of the fourth and fifth metacarpals with the hemicallotasis technique. Plast Reconstr Surg. 1997; 99:2061–2065.
Article5. Iwasawa M, Hayashi R, Matsuo K, Hirose T. The use of costal cartilage as a spacer in the treatment of congenital metacarpal fusion. Eur J Plast Surg. 1998; 11:138–140.
Article6. Lee KS, Park JW, Wie DG, Han SS. The surgical treatment of metacarpal synostosis. J Korean Soc Surg Hand. 1997; 2:363–368.7. Chung DW, Kim KT. Surgical management of congenital fourth and fifth metacarpal synostosis. J Korean Soc Surg Hand. 1999; 4:94–101.8. Gottschalk HP, Bednar MS, Moor M, Light TR. Metacarpal synostosis: treatment with a longitudinal osteotomy and bone graft substitute interposition. J Hand Surg Am. 2012; 37:2074–2081.
Article9. Jianmongkol S, Thammaroj T, Vipulakorn K. Congenital metacarpal synostosis treated by double bone blocks technique: a case report from Thailand. Hand Surg. 2005; 10:131–134.
Article10. Horii E, Miura T, Nakamura R, Nakao E, Kato H. Surgical treatment of congenital metacarpal synostosis of the ring and little fingers. J Hand Surg Br. 1998; 23:691–694.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of the Bilateral Congenital Radio - Ulnar Synostosis: A Case Report
- A Report of congenital Radio - Ulnar Synostosis Occurred in Brothers: One Case Associated with Klinefelter's Syndrome
- The Experience of Cystocele Repair with Monofilament polypropylene Mesh
- Reconstruction of a high-energy penetrating injury from the abdomen to the sacral area using a latissimus dorsi free flap with monofilament polypropylene mesh and pedicled flap rotation: a case report
- Congenital Distal Tibio-fibular Synostosis: Case Report
