J Korean Orthop Assoc.
2009 Apr;44(2):159-164.
Protocol for Administration of Prophylactic Antibiotics within One Hour before the Surgical Incision in Total Hip and Knee Replacement
- Affiliations
-
- 1Department of Orthopedics, Center for Joint Diseases, Chonnam National University Hwasun Hospital, Jeonnam, Korea. park5962@paran.com
Abstract
- PURPOSE
We aimed that compliance could be improved by new protocol ensuring the adequate timing of intravenous antibiotic delivery onto an already existing time out system used to ensure exact surgical site. MATERIALS AND METHODS: A group of 150 patients was administered prophylactic antibiotics just before entering operation room and performed only time-out protocol. Other group of 150 patients was administered prophylactic antibiotics directly after anesthetic induction and perfomed new protocol inclusive of checklist ensuring appropriate timing of antimicrobial prophylaxis. We compared mean time from prophylactic administration to surgical incision and compliance. RESULTS: The average time from administration of the antimicrobial prophylaxis to the surgical incision for patients who was performed only time-out protocol was 43 minutes and compliance was 60.6%. The average time from administration of the antimicrobial prophylaxis to the surgical incision for patients who was performed new protocol was 18 minutes and compliance was 100%. There was a significant difference in compliance of two groups. CONCLUSION: New protocol ensuring the adequate timing of intravenous antibiotic delivery combined with administration of the antimicrobial prophylaxis directly after anesthetic induction were effective and easily adaptable method to ensure compliance with appropriate timing of prophylactic antibiotics.
MeSH Terms
Figure
-

Fig. 1 New vertification protocol including the checklists of time-out and administration of preoperative antibiotics.

Fig. 2 Distribution of timing of antibiotic administration in patients before peforming new protocol by twenty-minute groupings.
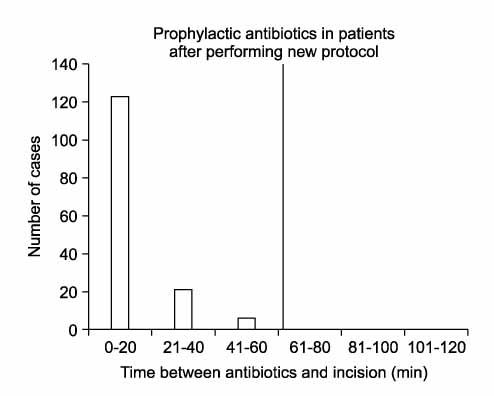
Fig. 3 Distribution of timing of antibiotic administration in patients after performing new protocol by fifteen-minute groupings.
Reference
-
1. Bhattacharyya T, Hooper DC. Antibiotic dosing before primary hip and knee replacement as a pay-for-performance measure. J Bone Joint Surg Am. 2007. 89:287–291.
Article2. Bratzler DW, Houck PM, Richards C, et al. Use of antimicrobial prophylaxis for major surgery: baseline results from the National Surgical Infection Prevention Project. Arch Surg. 2005. 140:174–182.3. Burke JF. The effective period of preventive antibiotic action in experimental incisions and dermal lesions. Surgery. 1961. 50:161–168.4. Classen DC, Evans RS, Pestotnik SL, Horn SD, Menlove RL, Burke JP. The timing of prophylactic administration of antibiotics and the risk of surgical-wound infection. N Engl J Med. 1992. 326:281–286.
Article5. Gyssens IC, Geerligs IE, Nannini-Bergman MG, Knape JT, Hekster YA, ver der Meer JW. Optimizing the timing of antimicrobial prophylaxis in surgery: an intervention study. J Antimicrob Chemother. 1996. 38:301–308.
Article6. Gyssens IC, Knape JT, Van Hal G, ver der Meer JW. The anaesthetist as determinant factor of quality of surgical antimicrobial prophylaxis. A survey in a university hospital. Pharm World Sci. 1997. 19:89–92.7. Hanssen AD, Osmon DR. The use of prophylactic antimicrobial agents during and after hip arthroplasty. Clin Orthop Relat Res. 1999. 369:124–138.
Article8. Harbarth S, Samore MH, Lichtenberg D, Carmeli Y. Prolonged antibiotic prophylaxis after cardiovascular surgery and its effect on surgical site infections and antimicrobial resistance. Circulation. 2000. 27:2916–2921.
Article9. Hecker MT, Aron DC, Patel NP, Lehmann MK, Donskey CJ. Unnecessary use of antimicrobials in hospitalized patients: current patterns of misuse with an emphasis on the antianaerobic spectrum of activity. Arch Intern Med. 2003. 163:972–978.10. Insall JN, Thompson FM, Brause BD. Two-stage reimplantation for the salvage of infected total knee arthroplasty. 1983. J Bone Joint Surg Am. 2002. 84:490.11. Matuschka PR, Cheadle WG, Burke JD, Garrison RN. A new standard of care: administration of preoperative antibiotics in the operating room. Am Surg. 1997. 63:500–503.12. Mauerhan DR, Nelson CL, Smith DL, et al. Prophylaxis against infection in total joint arthroplasty. One day of cefuroxime compared with three days of cefazolin. J Bone Joint Surg Am. 1994. 76:39–45.
Article13. Pavel A, Smith RL, Ballard A, Larsen IJ. Prophylactic antibiotics in clean orthopaedic surgery. J Bone Joint Surg Am. 1974. 56:777–782.
Article14. Polk HC Jr, Trachtenberg L, Finn MP. Antibiotic activity in surgical incisions. The basis for prophylaxis in selected operations. JAMA. 1980. 244:1353–1354.15. Silver A, Eichorn A, Kral J, et al. Timeliness and use of antibiotic prophylaxis in selected inpatient surgical procedures. The Antibiotic Prophylaxis Study Group. Am J Surg. 1996. 171:548–552.16. Whitehouse JD, Friedman ND, Kirkland KB, Richardson WJ, Sexton DJ. The impact of surgical-site infections following orthopedic surgery at a community hospital and a university hospital: adverse quality of life, excess length of stay, and extra cost. Infect Control Hosp Epidemiol. 2002. 23:183–189.
Article17. Wiggins CE, Nelson CL, Clarke R, Thompson CH. Concentration of antibiotics in normal bone after intravenous injection. J Bone Joint Surg Am. 1978. 60:93–96.
Article18. Windsor RE. Management of total knee arthroplasty infection. Orthop Clin North Am. 1991. 22:531–538.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Total Hip Replacement for Ankylosed and Deformed Hip
- The Effects of Preemptive Intravenous Ketorolac for Total Hip Replacement Patients
- Geometric Total Knee Arthroplasty: A Case Report
- Results of Primary Total Hip Arthroplasties Performed with a Mini-Incision or a Standard Incision
- Total Hip Replacement in Painful Stiff and Deformed Hips
