Periacetabular Osteotomy in Hip Dysplasia with Deformed Femoral Head
- Affiliations
-
- 1Department of Orthopedic Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jschang@amc.seoul.kr
- 2Department of Orthopedic Surgery, Ilsan Paik Hospital, University of Inje College of Medicine, Seoul, Korea.
Abstract
-
PURPOSE: To evaluate the results of a periacetabular osteotomy (PAO) combined with a femoral osteotomy (FO) for a dysplastic hip with a deformed femoral head.
MATERIALS AND METHODS
Thirteen hips with dysplasia and a deformed femoral head were followed up for more than 12 months. Eight hips were in the PAO group and 5 hips were in the PAO and FO group. The two groups were compared clinically according to the HHS (Harris hip score), pain and limping VAS (visual analogue scale), and radiologically according to the CEA (central edge angle of Wiberg), Tonnis angle (acetabular index of weight bearing surface), FHC (femoral head coverage), AA (acetabular angle of Sharp), DBSPFH (distance between symphysis pubis and femoral head) and AI (acetabular index of depth to width).
RESULTS
Regarding the clinical results, the PAO group showed improvement in the HHS from 66.5 preoperatively to 90.4 postoperatively (p=0.01) and the pain VAS from 6.7 to 1.9 (p=0.01). However, there was no significant improvement in limping (p=0.39). In the PAO with FO group, the HHS was improved from 78 to 91 (p=0.04). Radiologically, the CEA, Tonnis angle, FHC, AA and AI improved significantly but there were no significant improvement in the DBSPFH in the two groups. In addition, there was no significant clinical or radiological difference between the two groups.
CONCLUSION
Periacetabular osteotomy is recommended for dysplastic hips with deformed femoral head. A concomitant femoral osteotomy should be considered in hips with a severely deformed femoral head.
Figure
-
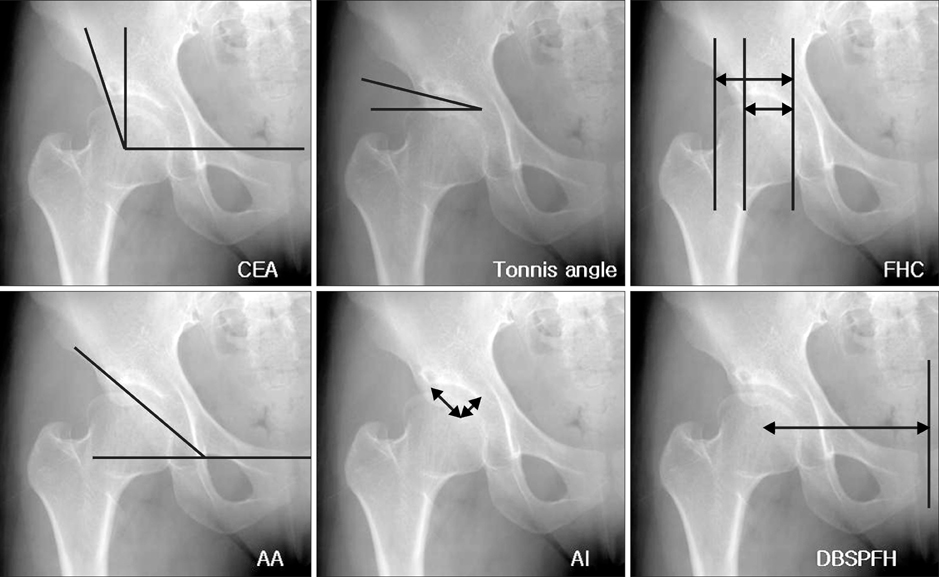
Fig. 1 Radiologic evaluations of the dysplastic hip. For the evaluation of coverage of femoral head, CE angle (CEA), Tonnis angle and femoral head coverage (FHC) were checked. To evaluate the inclination and depth of acetabulum, acetabular angle of Sharp (AA) and AI(acetabular index of depth to width). Finally to check the medialization of the femoral head, the distance between symphysis pubis and the femoral head was compared.

Fig. 2 Preoperative planning for periacetabular osteotomy and proximal femur osteotomy.

Fig. 3 Diagram of the dual approach. Anterior approach is modified Smith-Peterson approach and posterior approach is Kocher-Langenbock approach.
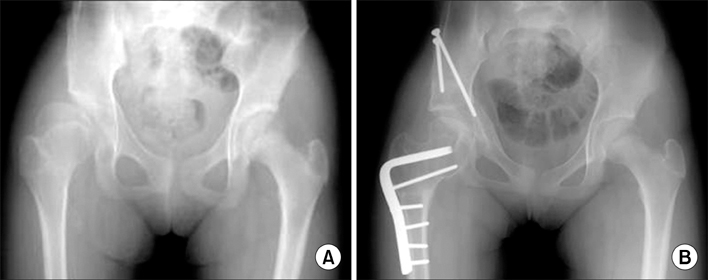
Fig. 4 41-year-old male patient with acetabular dysplasia. (A) Preoperative radiograph shows deformed femoral head, inclination of acetabulum and shollow acetabular coverage due to LCP sequelae. (B) MR arthrogram shows the labral tear of the acetabulm due to load concentration. (C) Postoperative radiograph shows excessive correction after periacetabular osteotomy. (D) Excessive retroversion of the acetabulum after periacetabular osteotomy which has caused impingement during hip flexion. Preoperatively the patient could flex the hip upto 130 degrees and sit on the posture of crossing both legs. As result of excessive retroversion, the patient can flex the hip upto just 110 degrees and have to sit unfolding the leg.

Fig. 5 (A) 25-year-old female patient who has acetabular dysplasia with deformed femoral head and coxa valga deformity. Preoperative anteroposterior radiographs in abduction and adduction position demonstrate the acceptable coverage and congruency in abduction position. (B) Postoperative radiograph shows satisfactory correction after periacetabular osteotomy and varus osteotomy of the proximal femur.
Reference
-
1. Brand RA. Hip osteotomies: a biomechanical consideration. J Am Acad Orthop Surg. 1997. 5:282–291.
Article2. Chang JS, Kwon KD, Shon HC. Bernese periacetabular osteotomy using dual approaches for hip dysplasias. J Korean Orthop Assoc. 2002. 37:226–232.
Article3. Chang JS, Park JH, Park HG, Lee SH, Kim KY. Bernese periacetabular osteotomy for hip dysplasia. J Korean Hip Soc. 1998. 10:141–148.4. Clohisy JS, Nunley RM, Curry MC, Schoenecker PL. Periacetabulr osteotomy for the treatment of acetabular dysplasia associated with major aspherical femoral head deformities. J Bone Joint Surg Am. 2007. 89:1417–1423.5. Cooperman DR, Wallensten R, Stulberg SD. Acetabular dysplasia in the adult. Clin Orthop Relat Res. 1983. 175:79–85.
Article6. Ganz R, Klaue K, Vinh TS, Mast JW. A new periacetabular osteotomy for the treatment of hip dysplasias: technique and preliminary results. 1988. Clin Orthop Relat Res. 2004. 418:3–8.7. Ian K. Acetabular dysplasia: the acetabular angle. J Bone Joint Surg Br. 1961. 43:268–272.8. Matta JM, Stover MD, Siebenrock K. Periacetabular osteotomy through the Smith-Petersen approach. Clin Orthop Rel Res. 1999. 363:21–32.9. Murphy S, Ganz R, Müller M. The prognosis of untreated dyplasia of the hip. A study of radiographic factors that predict the out come. J Bone Joint Surg Am. 1995. 77:985–989.10. Murphy S, Millis M, Hall J. Surgical correction of acetabular dysplasia in the adult. A Boston experience. Clin Orthop Relat Res. 1999. 363:38–44.11. Nakamura S, Ninomiya S, Morimoto S, Moro T, Takatori Y. Combined intertrochanteric valgus and rotational acetabular osteotomy. Clin Orthop Relat Res. 2001. 384:176–188.
Article12. Pogliacomi F, Stark A, Wallensten R. Periacetabular osteotomy. Good pain relief in symptomatic hip dysplasia, 32 patients followed for 4 years. Acta Orthop. 2005. 76:67–74.13. Sienbenrock KA, Schöll E, Lottenbach M, Ganz R. Bernese periacetabular osteotomy. Clin Orthop Relat Res. 1999. 363:9–20.14. Tonnis D. Normal values of the hip joint for the evaluation of X-rays in children and adults. Clin Orthop Relat Res. 1976. 119:39–47.15. Tonnis D, Arning A, Bloch M. Triple pelvic osteotomy. J Pediatr Orthop B. 1994. 3:54–67.16. Trumble SJ, Mayo KA, Mast JW. The periacetabular osteotomy. Minimal 2-year follow-up in more than 100 hips. Clin Orthop Relat Res. 1999. 363:54–63.17. Weinstein SL. Natural history of congenital hip dislocation (CHD) and hip dysplasia. Clin Orthop Relat Res. 1987. 225:62–76.18. Wiberg G. Self operation in congenital dysplasia of the acetabulum and in subluxation and dislocation of the hip. J Bone Joint Surg Am. 1953. 35:65–80.
