J Korean Rheum Assoc.
2009 Dec;16(4):312-317.
Bronchiolitis Obliterans with Organizing Pneumonia (BOOP) in a Patient with Rheumatoid Arthritis
- Affiliations
-
- 1Division of Rheumatology, Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. pkyungsu@catholic.ac.kr
Abstract
- Interstitial lung disease (ILD) is one of the common extra-articular manifestations of rheumatoid arthritis (RA). Bronchiolitis obliterans with organizing pneumonia (BOOP) is one type of ILD, and this is characterized by the proliferation of granulation tissue in the bronchioles, alveolar ducts and some alveoli and interstitial infiltration by chronic inflammatory cells. It develops as a manifestation of RA or as a side effect of anti-rheumatic drugs in patients with RA. We experienced a 41-year-old female patient with RA who developed BOOP during the treatment with methotrexate and bucillamine. She presented with cough and sputum for several months and pleuritic chest pain for one week. The chest radiograph showed bilateral multifocal consolidations. She received thoracoscopic biopsy and her pulmonary infiltrations resolved after the treatment with corticosteroid.
MeSH Terms
Figure
-

Fig. 1. The chest PA shows bilateral multiple consolidations with ill-defined margins.
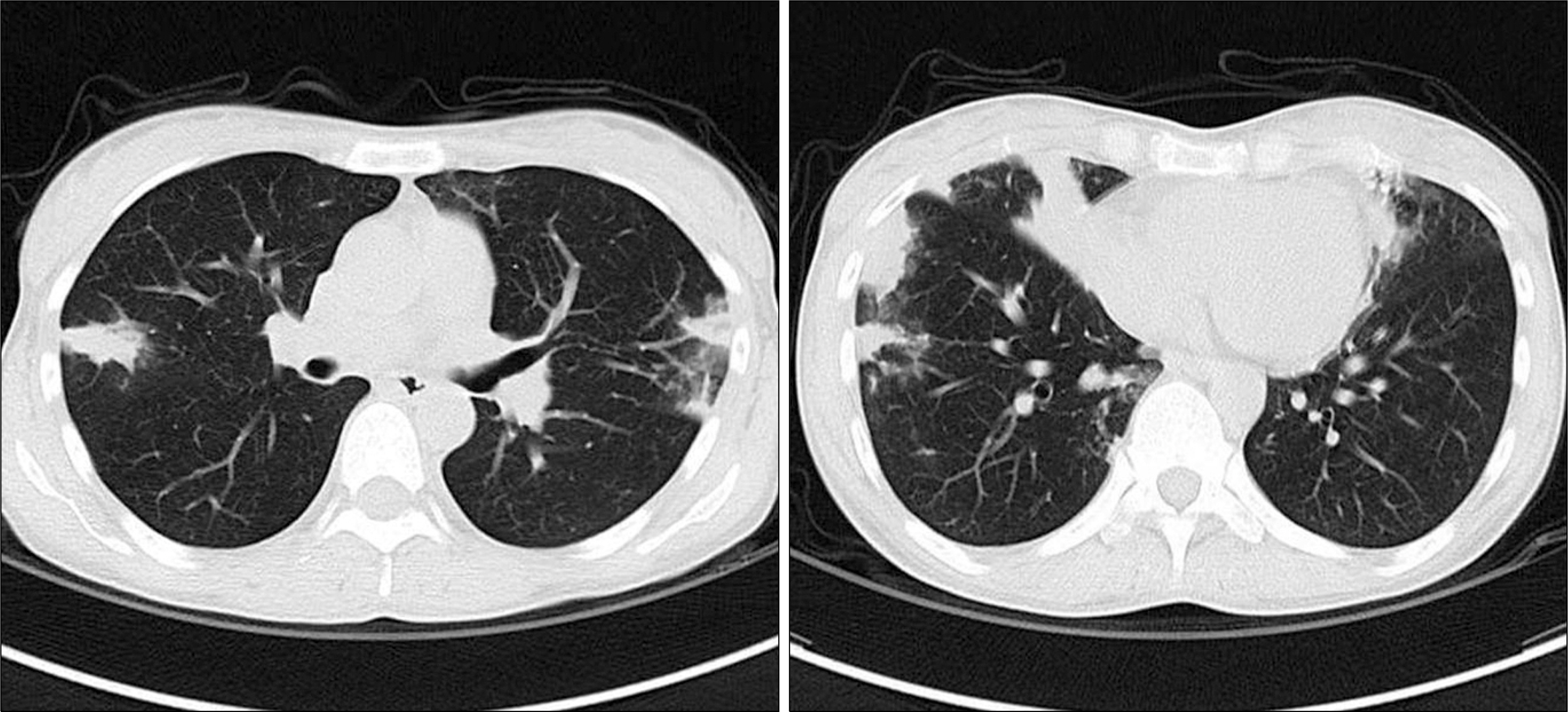
Fig. 2. The chest HRCT shows multiple peripheral macronodules and patchy consolidation in both the mid-lung and lower lung field.
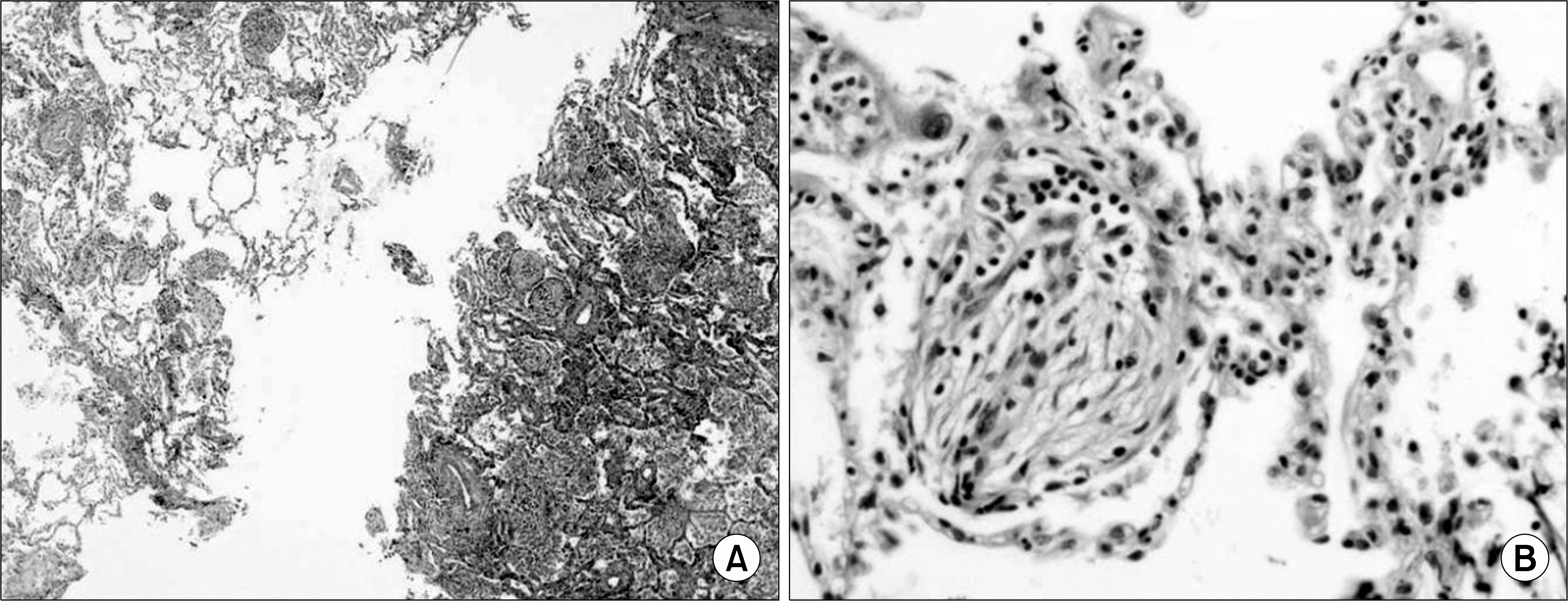
Fig. 3. The video-assisted thoracoscopic wedge resection specimen (H&E stain) shows interstitial inflammatory cell infiltration and granulation tissue occupying the bronchioles and alveolar ducts (A, ×12.5) and myofibroblastic tissue filling the alveolar cavity (B, ×400).
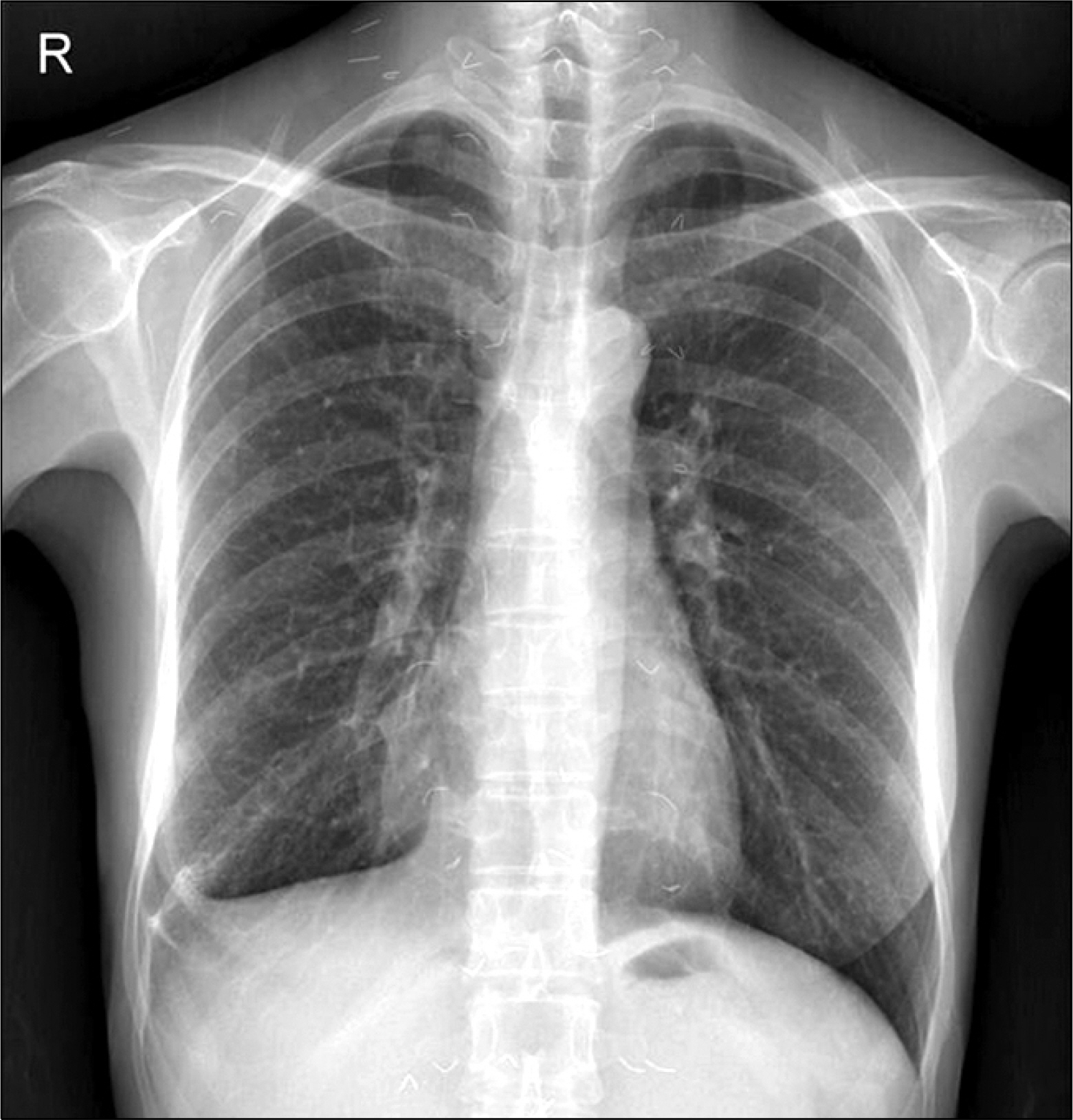
Fig. 4. The chest PA taken one month after the beginning of corticosteroid treatment shows resolution of the bilateral multifocal consolidations. Post surgical scarring is also noted at the right costo-phrenic angle area.
Reference
-
References
1. Carmona L, Gonzalez-Alvaro I, Balsa A, Angel Belmonte M, Tena X, Sanmarti R. Rheumatoid arthritis in Spain: occurrence of extra-articular manifestations and estimates of disease severity. Ann Rheum Dis. 2003; 62:897–900.
Article2. Anaya JM, Diethelm L, Ortiz LA, Gutierrez M, Citera G, Welsh RA, et al. Pulmonary involvement in rheumatoid arthritis. Semin Arthritis Rheum. 1995; 24:242–54.
Article3. Colby TV. Pathologic aspects of bronchiolitis obliterans organizing pneumonia. Chest. 1992; 102:S38–43.
Article4. Lee YH, Kim YR, Ji JD, Shim JJ, Kang KH, Lee JH, et al. A case of BOOP developed during bucillamine treatment for rheumatoid. Korean J Intern Med. 2001; 16:36–9.
Article5. Kim SG, Kim JY, Lee YH, Cho JY, Kim HK, Song GG. A case of bronchiolitis obliterans organizing pneumonia anteceded by rheumatoid arthritis. Tuberculosis and Respiratory Disease. 1996; 43:630–6.
Article6. American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias. Am J Respir Crit Care Med. 2002; 165:277–304.7. Kim DS. Interstitial lung disease in rheumatoid arthritis: recent advances. Curr Opin Pulm Med. 2006; 12:346–53.
Article8. Sara AG, Hamdan AJ, Hanaa B, Nawaz KA. Bronchiolitis obliterans organizing pneumonia: pathogenesis, clinical features, imaging and therapy review. Ann Thorac Med. 2008; 3:67–75.
Article9. Ippolito JA, Palmer L, Spector S, Kane PB, Gorevic PD. Bronchiolitis obliterans organizing pneumonia and rheumatoid arthritis. Semin Arthritis Rheum. 1993; 23:70–8.
Article10. Kajiya T, Kuroda A, Hokonohara D, Tei C. Radiographic appearance of bronchiolitis obliterans organizing pneumonia (BOOP) developing during Bucillamine treatment for rheumatoid arthritis. Am J Med Sci. 2006; 332:39–42.
Article11. Cho I, Mori S, Imamura F, Kiyofuji C, Sugimoto M. Methotrexate pneumonia lacking dyspnea and radiographic interstitial patterns during treatment for early rheumatoid arthritis: bronchoalveolar lavage and transbronchial lung biopsy in a differential diagnosis. Mod Rheumatol. 2007; 17:256–61.
Article12. Ulubas B, Sahin G, Ozer C, Aydin O, Ozgur E, Apaydin D. Bronchiolitis obliterans organizing pneumonia associated with sulfasalazine in a patient with rheumatoid arthritis. Clin Rheumatol. 2004; 23:249–51.13. Imokawa S, Colby TV, Leslie KO, Helmers RA. Methotrexate pneumonitis: review of the literature and histopathological findings in nine patients. Eur Respir J. 2000; 15:373–81.
Article14. Hsu PC, Lan JL, Hsieh TY, Jan YJ, Huang WN. Methotrexate pneumonitis in a patient with rheumatoid arthritis. J Microbiol Immunol Infect. 2003; 36:137–40.15. Kaushik P, Cooper ES, Banda VR, Vatsavai SR, Kaushik R. Bronchiolitis obliterans with organizing pneumonia in rheumatoid arthritis–a fatal case and short review of literature. Rheumatol Int. 2005; 25:391–3.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Bronchiolitis Obliterans Organizing Pneumonia anteceded by Rheumatoid Arthritis
- A case of bronchiolitis obliterans organizing pneumonia in patient with systemic lupus erythematosus
- Two Cases of Bronchiolitis Obliterans Organizing Pneumonia treated with Steroid and Cyclosporine therapy
- Polymyositis Associated with Bronchiolitis Obliterans Organizing Pneumonia
- Diffuse Micronodular Pattern of Bronchiolitis Obliterans Organizing Pneumonia: A Case Report
