Common Misconceptions or Misdiagnosis in Shoulder Disorders
- Affiliations
-
- 1Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hahc78@hanmail.net
Abstract
- Many patients, physicians and even orthopedic surgeons commonly have misconceptions about several shoulder disorders, so they misdiagnose these diseases and treat patients inappropriately. In this article, we describe some common misconceptions and misdiagnosis in shoulder disorders; such as rotator cuff disease, SLAP lesion, clavicle fracture et al. It will be helpful to understand how these disorders can be approached and managed.
Figure
-

Fig. 1. Glenohumeral AP view of right shoulder shows sclerosis and irregularity of greater tuberosity.

Fig. 2. Acromiohumeral distance is less than 7 mm.
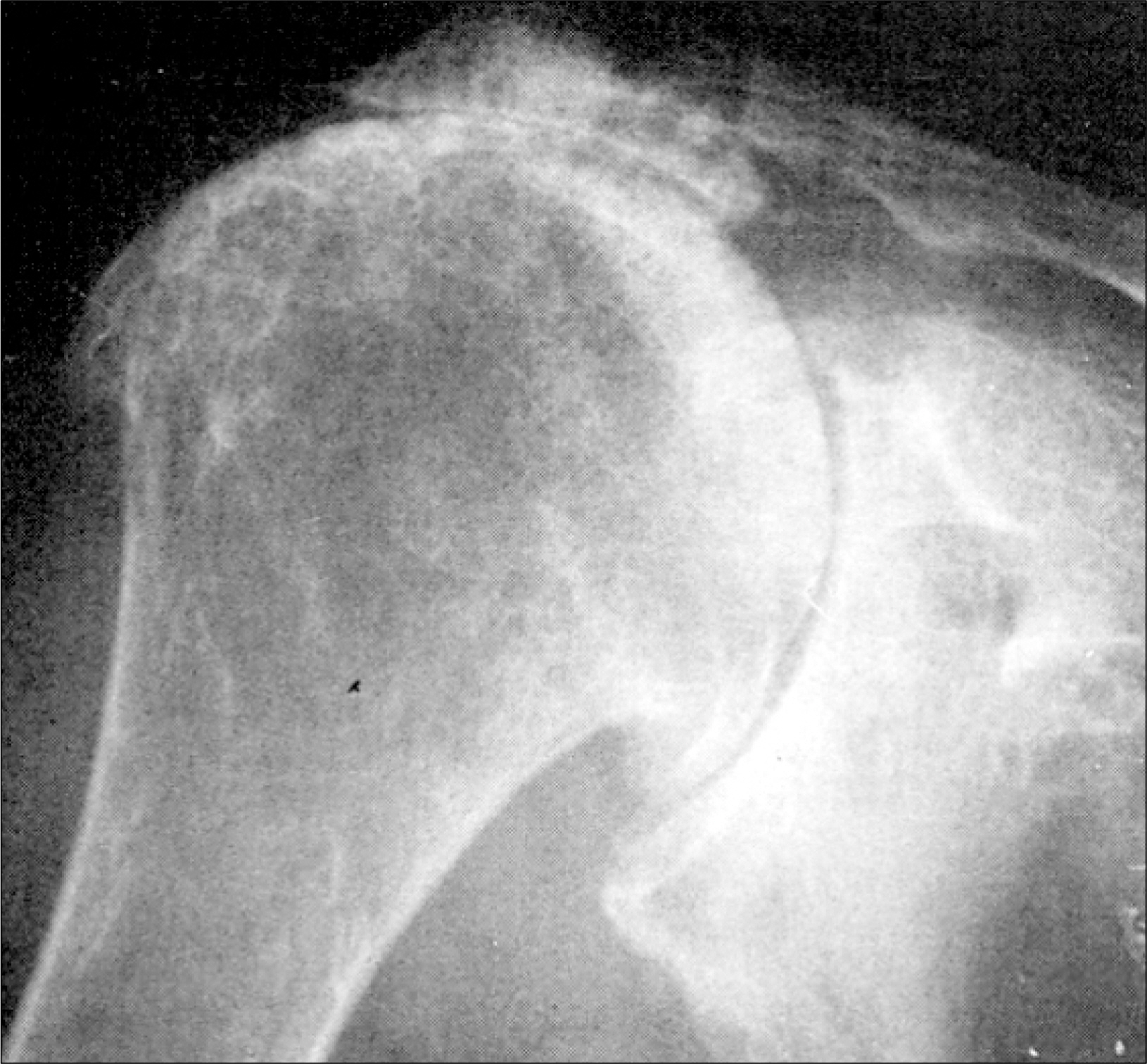
Fig. 3. Cuff tear arthropathy showing femoralization of the proximal end of the humerus and acetabula- rization of the coracoacromial arch and glenoid.
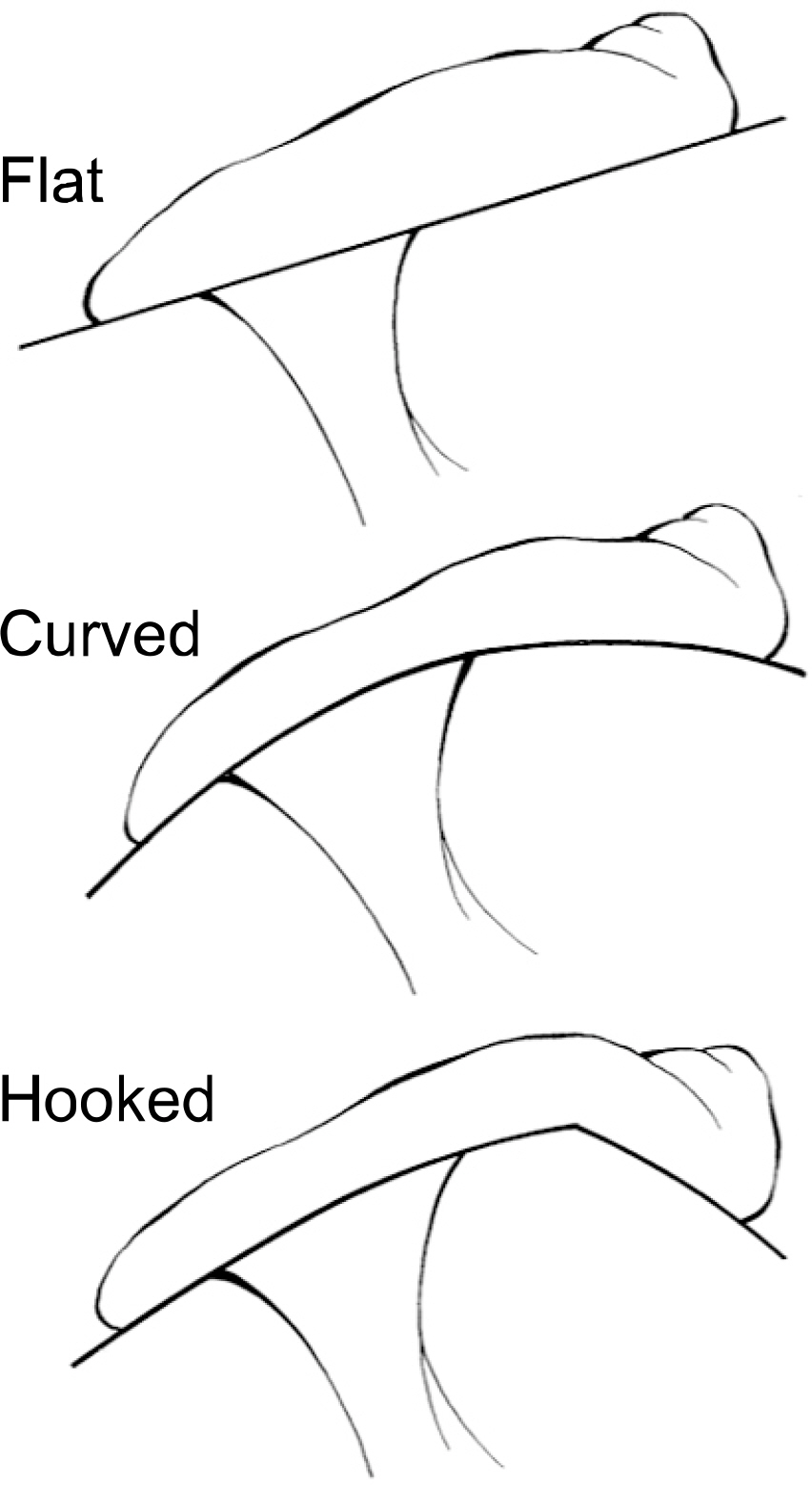
Fig. 4. Acromion morphology.
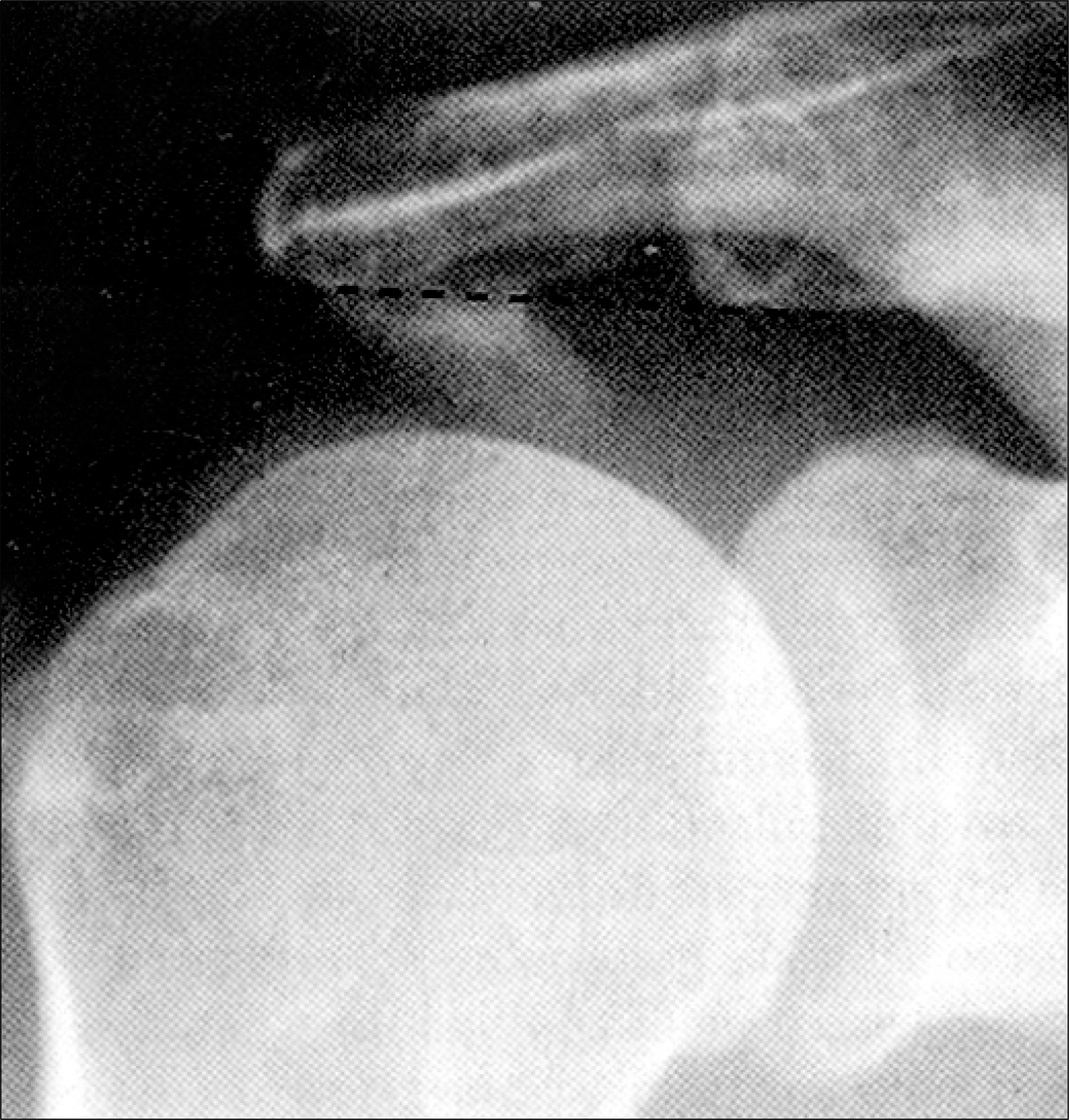
Fig. 5. 30-degree caudal tilt radiograph depicting anterior- inferior projection of an acromial spur. The solid line designates the anterior cortical margin of the distal clavicle.
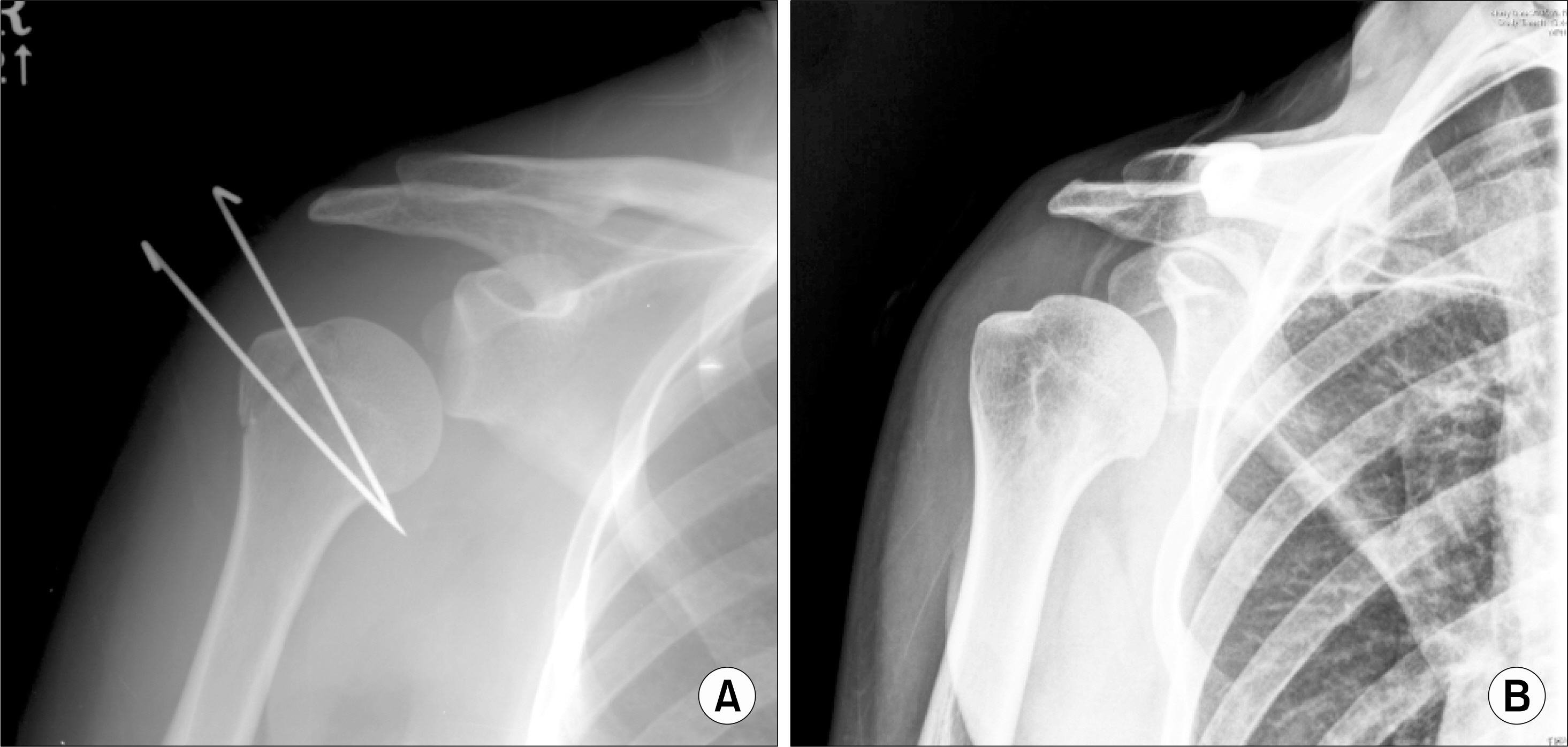
Fig. 6. (A) Inferior subluxation of humeral head on glenohumeral AP view taken 2 weeks after operation. (B) Inferior subluxation of humeral head on glenohumeral AP view taken 2 weeks after arthroscopic Bankart repair.
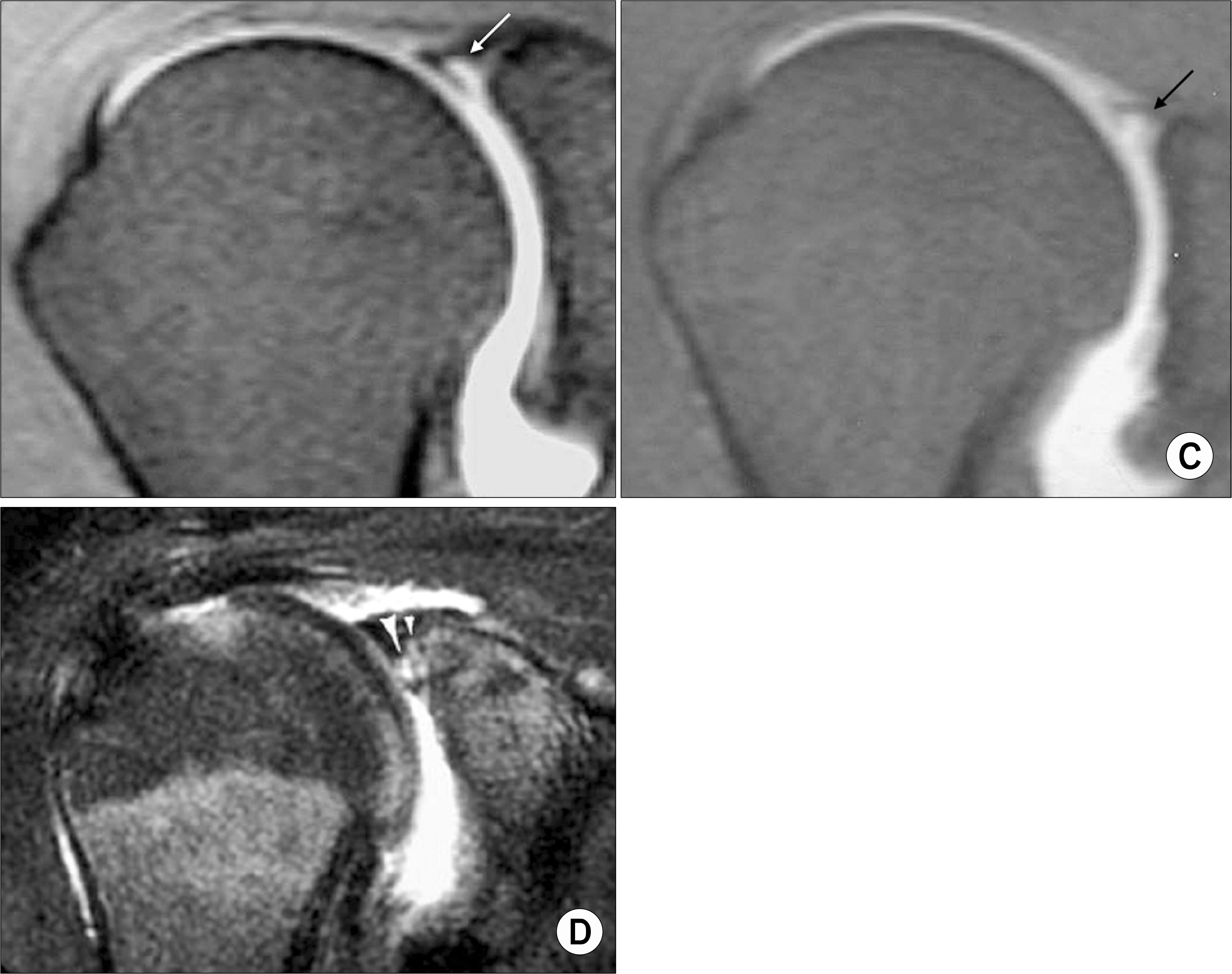
Fig. 7. (A) (left) High signal intensity not extending to posterior portion of superior labrum, (right) high signal intensity (arrow) in posterior third of superior labrum. (B) (left) Medially curved high signal intensity, (right) laterally curved high signal intensity. (C) (left) Band-like high signal intensity (arrow) with smooth margin, (right) globular and irregular high signal intensity (arrow) in superior labrum. (D) Two high-signal intensity lines (arrowheads) in the superior labrum; the more lateral line (large arrowhead) represents the SLAP tear.
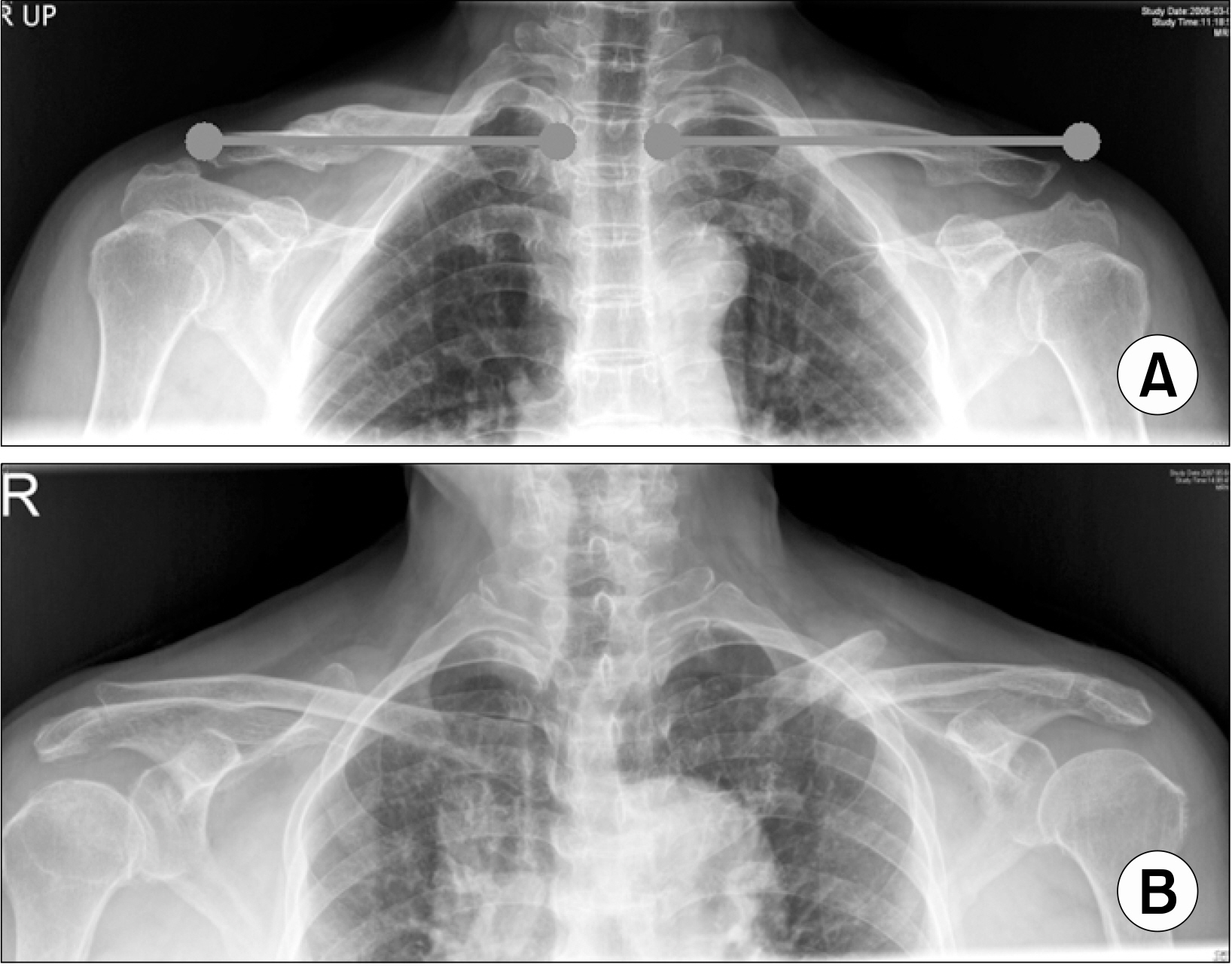
Fig. 8. (A) Shortening of right clavicle after conservative treatment. (B) Malunion of left clavicle.
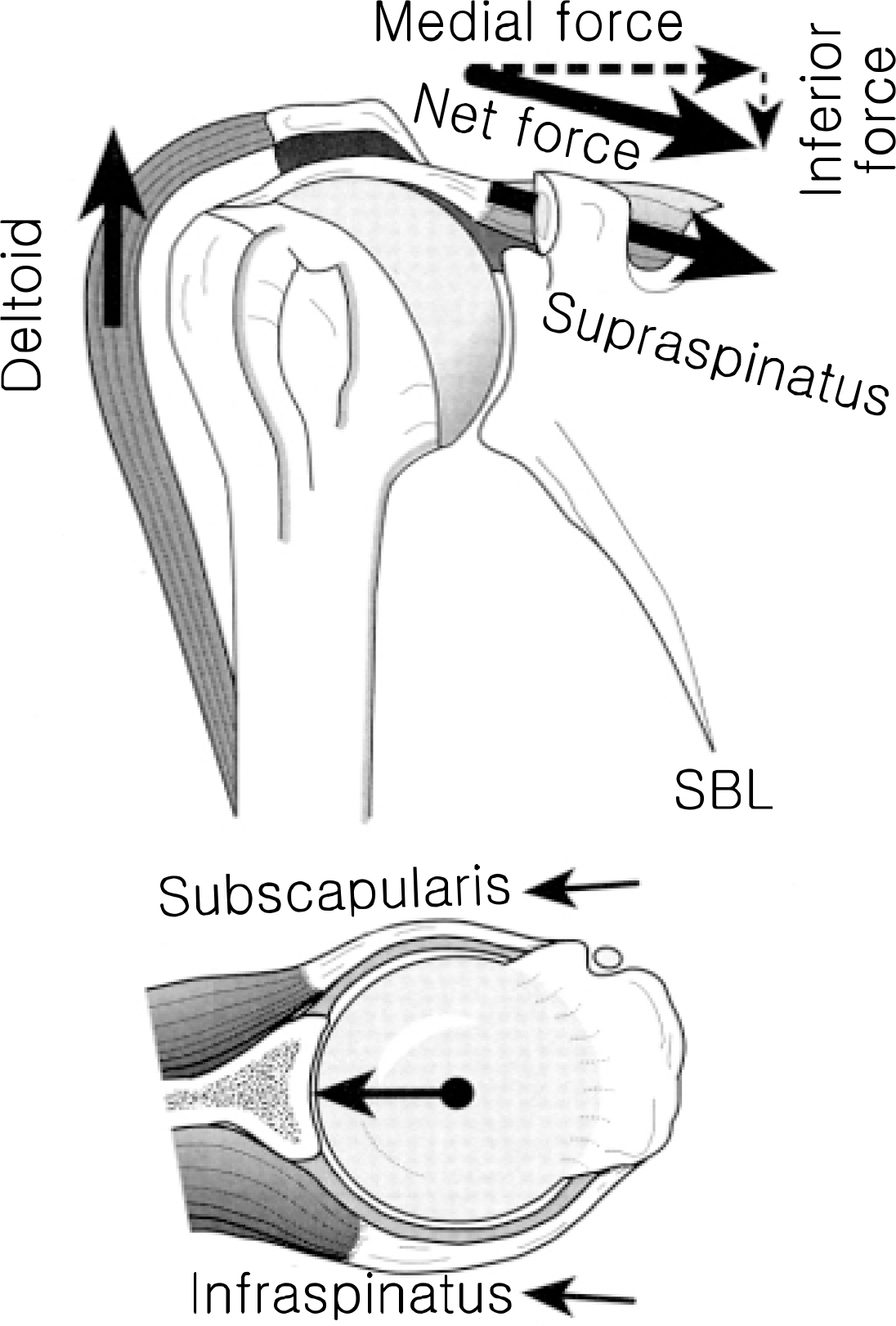
Fig. 9. Concavity compression. The supraspinatus muscle is not optimally oriented to depress the head of the humerus against upward pull of the deltoid because the inferiorly directed component of the supraspinatus force is small. Instead, the humeral head is stabilized in the concave glenoid fossa by the compressive action of the cuff muscles. (Modified from Matsen FA III, Lippitt SB, Sidles JA, Harryman DT II. Practical evaluation and management of the shoulder. Philadelphia: WB Saunders, 1994).
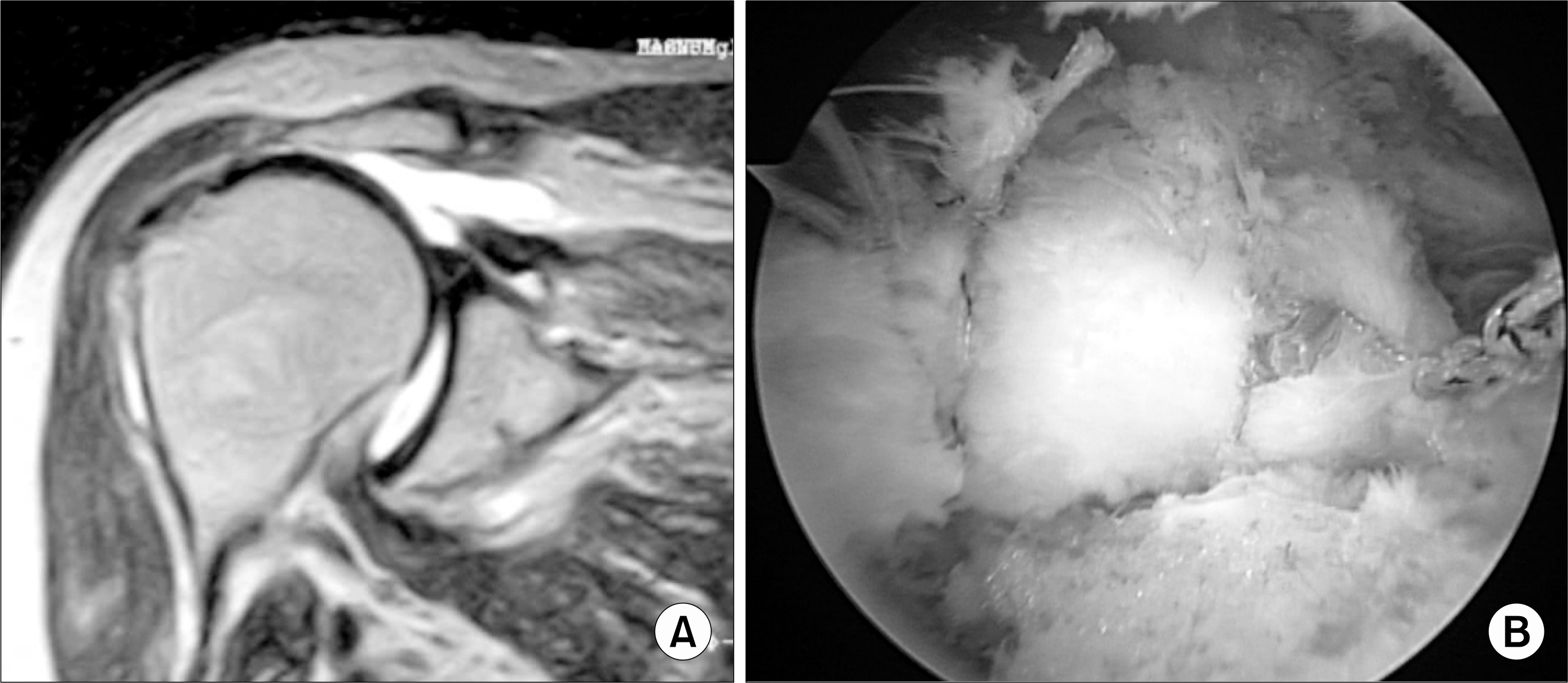
Fig. 10. (A) Massive rotator cuff tear on MRI scan of right shoulder. (B) Even massive rotator cuff tear can be repaired satisfactorily.

Fig. 11. Although massive tear is repaired incompletely, it can be helpful to relieve symptoms.
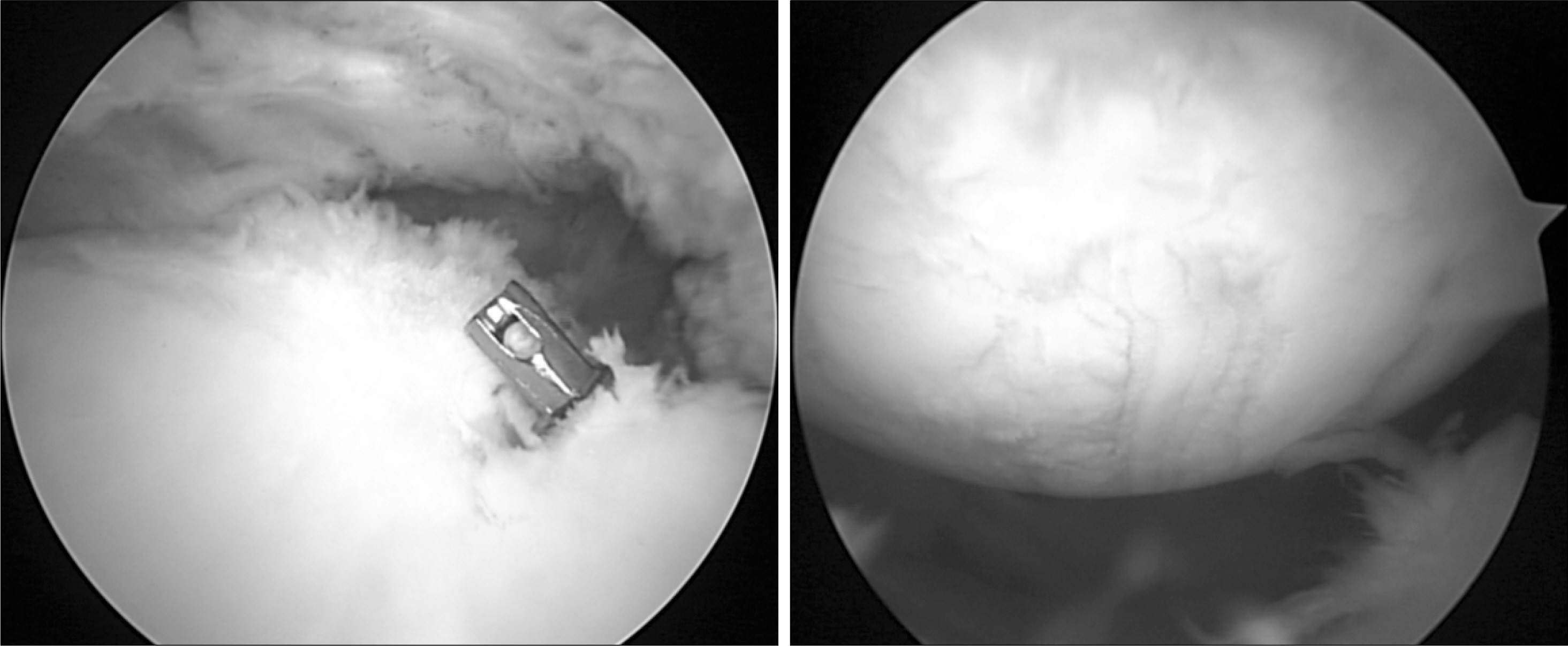
Fig. 12. Articular cartilage was injured by extruded metal anchor.

Fig. 13. Blood clot on torn margin suggests acute on chronic rotator cuff tear.
Reference
-
1). Cotton FJ. Subluxation of the shoulder-downward. Boston Med Surg J. 1921. 185:405–7.2). Kessel L. Injuries of the shoulder. In:. Wilson JN, editor. ed.Fractures and joint injuries. 6th ed.p. 545. New York, Churchil Livingstone;1982.3). Mocckel BH., Warren RF., Dines DM., Altchek DW. The unstable shoulder arthroplasty. In: Friedman RJ, ed. Arthroplasty of the shoulder. p. 262, New York, Thieme Medical Publishers. 1994.4). Neer CS II. Shoulder reconstruction. p. 371, Philadelphia, WB Saunders Company. 1990.5). Neer CS II. Displaced proximal humerus fractures. Part II. Treatment of a three-part and four-part displacement. J Bone Joint Surg Am. 1970. 52A:1090–103.6). Pritchett JW. Inferior subluxation of the humeral head after trauma or surgery. J Shoulder Elbow Surg. 1997. 6:356–9.
Article7). Smith DK., Chopp TM., Aufdemorte TB., Witkowski EG., Jones RC. Sublabral recess of the superior glenoid labrum: study of cadavers with conventional nonenhanced MR imaging, MR arthrography, anatomic dissection, and limited histologic examination. Radiology. 1996. 201:251–6.
Article8). Tuite MJ., Cirillo RL., De Smet AA., Orwin JF. Superior labrum anterior-posterior (SLAP) tears: evaluation of three MR signs on T2-weighted images. Radiology. 2000. 215:841–5.
Article9). Chandnani VP., Yeager TD., DeBerardino T., Chris-tensen K., Gagliardi JA., Heitz DR, et al. Glenoid labral tears. Prospective evaluation with MR imaging, MR arthrography and CT arthrography. Am J Roentgenol. 1993. 161:1229–35.10). Reuss BL., Schwartzberg R., Zlatkin MB., Cooperman A., Dixon JR. Magnetic resonance imaging accuracy for the diagnosis of superior labrum anterior-posterior lesions in the community setting: eighty-three arthroscopically confirmed cases. J Shoulder Elbow Surg. 2006. 15:580–5.
Article11). Jones GL., Galluch DB. Clinical assessment of superior glenoid labral lesions: a systematic review. Clin Orthop Relat Res. 2007. 455:45–51.12). Franceschi F., Longo UG., Ruzzini L., Rizzello G., Maffulli N., Denaro V. No advantages in repairing a type II superior labrum anterior and posterior (SLAP) lesion when associated with rotator cuff repair in patients over age 50: a randomized controlled trial. Am J Sports Med 2007 Oct 16; [Epub ahead of print].13). Lazarides S., Zafiropoulos G. Conservative treatment of fractures at the middle third of the clavicle: the relevance of shortening and clinical outcome. J Shoulder Elbow Surg. 2006. 15:191–4.
Article14). Neer CS II. Anterior acromioplasty for the chronic impingement syndrome in the shoulder. J Bone Joint Surg Am. 1972. 54:41–50.
Article15). Bigliani LU., Morrison D., April EW. The morphology of the acromion and its relationship to the rotator cuff tears. Orthop Trans. 1986. 10:228.16). Sharkey NA., Marder RA. The rotator cuff opposes superior translation of the humeral head. Am J Sports Med. 1995. 23:270–5.
Article17). Thompson WO., Debski RE., Boardman ND 3rd., Taskiran E., Warner JJ., Fu FH, et al. A biomechanical analysis of rotator cuff deficiency in a cadaveric model. Am J Sports Med. 1996. 24:286–92.
Article18). Wuelker N., Plitz W., Roetman B. Biomechanical data concerning the shoulder impingement syndrome. Clin Orthop Relat Res. 1994. 303:242–9.
Article19). Burkhart SS., Barth JR., Richards DP., Zlatkin MB., Larsen M. Arthroscopic repair of massive rotator cuff tears with stage 3 and 4 fatty degeneration. Arthroscopy. 2007. 23:347–54.
Article20). Boileau P., Baque F., Valerio L., Ahrens P., Chuinard C., Trojani C. Isolated arthroscopic biceps tenotomy or tenodesis improves symptoms in patients with massive irreparable rotator cuff tears. J Bone Joint Surg Am. 2007. 89:747–57.
Article21). Lam F., Mok D. Open repair of massive rotator cuff tears in patients aged sixty-five years or over: is it worthwhile? J Shoulder Elbow Surg. 2004. 13:517–21.
Article22). Klinger HM., Steckel H., Ernstberger T., Baums MH. Arthroscopic debridement of massive rotator cuff tears: negative prognostic factors. Arch Orthop Trauma Surg. 2005. 125:261–6.
Article
