Analysis of Clinical Outcome and Prognosis for Lisfranc Joint Fracture and Dislocation according to the Injury Mechanism and Treatment Method
- Affiliations
-
- 1Department of Orthopaedic Surgery, Dankook University Hospital, Cheonan, Korea. m3artist@hanmail.net
- KMID: 2333480
- DOI: http://doi.org/10.14193/jkfas.2014.18.3.124
Abstract
- PURPOSE
The purpose of this study was to assess the treatment outcomes and prognosis of Lisfranc joint fracture and dislocation according to the mechanism of injury and treatment method.
MATERIALS AND METHODS
Twenty six patients with Lisfranc fracture-dislocation who had been treated surgically were included in this retrospective study. The patients were divided into two groups according to mechanism of injury: direct crushing injury (16 patients) and indirect rotational or compressive injury (10 patients). The patients were also divided into three groups according to the surgical methods. The parameters used were radiographic evaluation, patients' subjective satisfaction levels, length of hospital stay, and the American Orthopaedic Foot and Ankle Society (AOFAS) midfoot score. Statistical analysis was performed.
RESULTS
The mean postoperative AOFAS midfoot score was 78.7. The mean length of stay was 39.6 days. Statistically significant differences in subjective satisfaction, AOFAS midfoot score, and length of hospital stay were observed between the two groups (p<0.05). However, no significance differences were observed between the three groups who were divided according to the different surgical methods (p>0.05).
CONCLUSION
Mechanism of trauma and the severity of soft-tissue injury were significant prognostic factors affecting the surgical outcomes of Lisfranc joint fracture and dislocation.
Figure
-

Figure 1. (A) Preoperative anteroposterior radiograph of left foot showed fracture and dislocation of Lisfranc joint. (B) Postoperative anteroposterior radiograph of left foot showed well reduced fracture and dislocation with cannulated screw fixation.
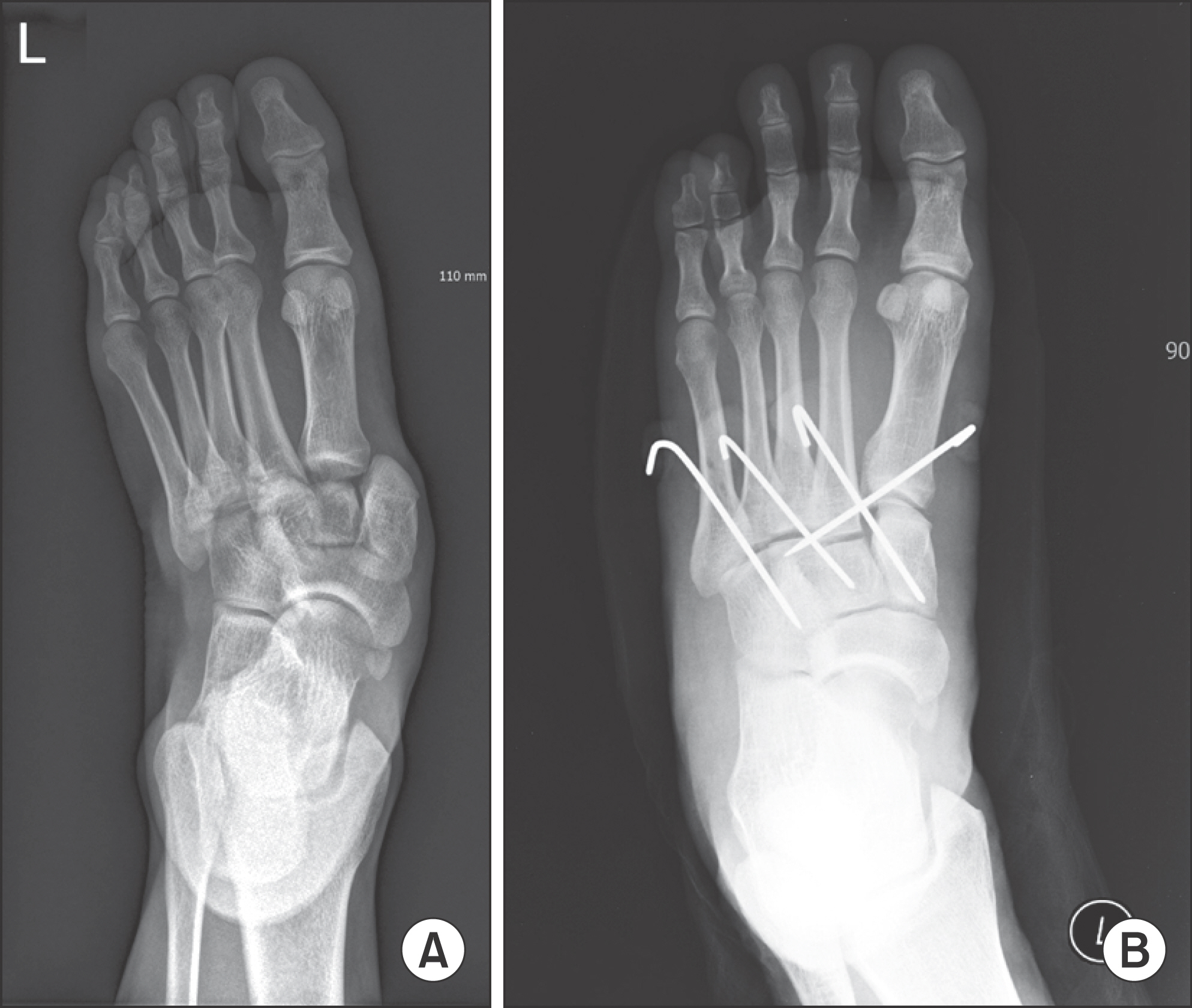
Figure 2. (A) Preoperative anteroposterior radiograph of left foot showed fracture and dislocation of Lisfranc joint. (B) Postoperative anteroposterior radiograph of left foot showed well reduced fracture and dislocation of Lisfranc joint using percutaneous K-wire fixation.

Figure 3. (A) Preoperative anteroposterior radiograph of right foot showed fracture and dislocation of Lisfranc joint. (B) Preoperative lateral radiograph of right foot showed fracture and dislocation of Lisfranc joint. (C) Postoperative anteroposterior radiograph of right foot showed well reduced fracture and dislocation of Lisfranc joint using Ilizarov external fixator. (D) Postoperative lateral radiograph of right foot showed well reduced fracture and dislocation of Lisfranc joint using Ilizarov external fixator.
Reference
-
1.Myerson MS., Fisher RT., Burgess AR., Kenzora JE. Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot Ankle. 1986. 6:225–42.
Article2.Hardcastle PH., Reschauer R., Kutscha-Lissberg E., Schoffmann W. Injuries to the tarsometatarsal joint. Incidence, classification and treatment. J Bone Joint Surg Br. 1982. 64:349–56.
Article3.Kuo RS., Tejwani NC., Digiovanni CW., Holt SK., Benirschke SK., Hansen ST Jr, et al. Outcome after open reduction and internal fixation of Lisfranc joint injuries. J Bone Joint Surg Am. 2000. 82:1609–18.
Article4.Mulier T., Reynders P., Dereymaeker G., Broos P. Severe Lisfrancs injuries: primary arthrodesis or ORIF? Foot Ankle Int. 2002. 23:902–5.
Article5.Schepers T., Oprel PP., Van Lieshout EM. Influence of approach and implant on reduction accuracy and stability in lisfranc fracture-dislocation at the tarsometatarsal joint. Foot Ankle Int. 2013. 34:705–10.
Article6.Adelaar RS. The treatment of tarsometatarsal fracture-dislocation. Inst Cours Lect. 1990. 39:141–5.7.Heckman JD. Fracture and dislocation of the foot. Rockwood CA, Green DP, Bucholz RD, editors. editors.Rockwood and Green’s fractures in adults. 4th ed.Philadelphia: Lippincott-Raven;1996. p. 2363–73.8.Thordarson DB. Fractures of the midfoot and forefoot. Myer-son MS, editor. editor.Foot and ankle disorders. Philadelphia: Saunders;2000. p. 1265–80.9.Perugia D., Basile A., Battaglia A., Stopponi M., De Simeonibus AU. Fracture dislocations of Lisfranc’s joint treated with closed reduction and percutaneous fixation. Int Orthop. 2003. 27:30–5.
Article10.Myerson MS. The diagnosis and treatment of injury to the tarsometatarsal joint complex. J Bone Joint Surg Br. 1999. 81:756–63.
Article11.Richter M., Wippermann B., Krettek C., Schratt HE., Hufner T., Therman H. Fractures and fracture dislocations of the midfoot: occurrence, causes and long-term results. Foot Ankle Int. 2001. 22:392–8.
Article12.Thompson MC., Mormino MA. Injury to the tarsometatarsal joint complex. J Am Acad Orthop Surg. 2003. 11:260–7.
Article13.Ahn GY., Yoo YS., Yun HH., Yun KP., Nam IH. Treatment of fracture and dislocation of Lisfranc joint with limited open reduction, pin fixation and Ilizarov external fixation. J Korean Foot Ankle Soc. 2004. 8:182–90.14.Demirkale I., Tecimel O., Celik I., Kilicarslan K., Ocguder A., Dogan M. The effect of the Tscherne injury pattern on the outcome of operatively treated Lisfranc fracture dislocations. Foot Ankle Surg. 2013. 19:188–93.
Article
