Obstet Gynecol Sci.
2016 Jul;59(4):319-322. 10.5468/ogs.2016.59.4.319.
Successful term delivery cases of trans-abdominal cervicoisthmic cerclage performed at more than 18 weeks of gestation
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. kbongchun@hanmail.net
- KMID: 2329055
- DOI: http://doi.org/10.5468/ogs.2016.59.4.319
Abstract
- A 38-year-old nulliparous woman was referred to our clinic because of cervical incompetence at 19 weeks of gestation. Trans-abdominal cervicoisthmic cerclage was performed after failure of modified Shirodkar cerclage operation in the patient at 21 weeks of gestation via a laparotomic approach. Another 38-year-old patient, who underwent loop electrosurgical excision procedure conization for treatment of cervical dysplasia 4 years ago, presented for cervical incompetence. At 18 weeks of gestation, we performed trans-abdominal laparotomic cervicoisthmic cerclage without any post-operative complications. During antenatal follow-up, there were no obstetrical co-morbidities and finally she gave birth to a healthy infant at full term by cesarean section. We report two cases of women who underwent trans-abdominal cervicoisthmic cerclage surgery because of cervical incompetence as they were not suitable for transvaginal cervical cerclage. Both patients successfully maintained their pregnancy until full term after undergoing transabdominal cervicoisthmic cerclage at more than 18 weeks of gestation.
MeSH Terms
Figure
-
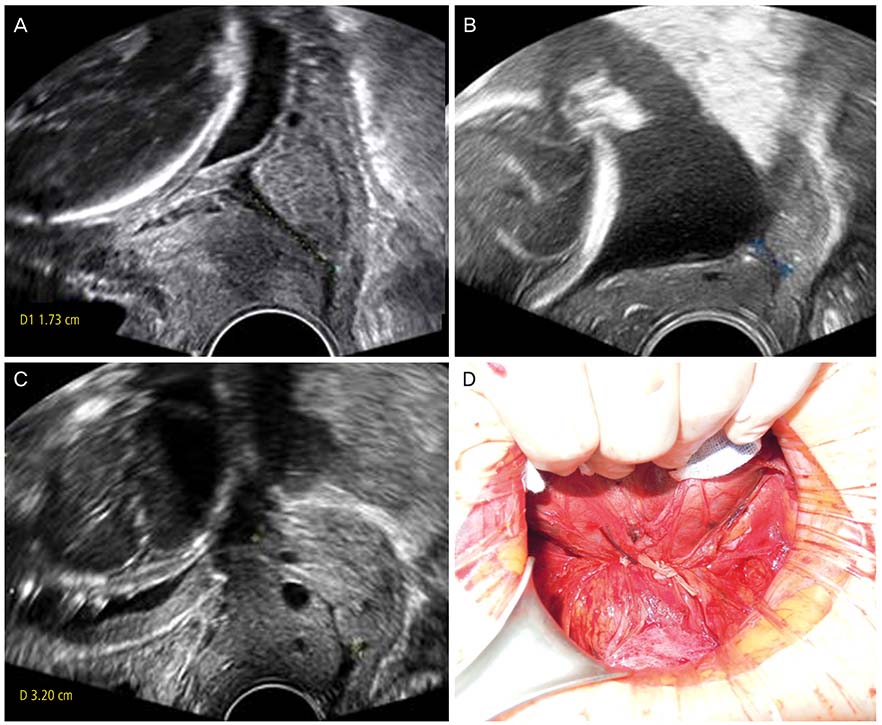
Fig. 1 Serial changes in cervical length of the patient (case 1). (A) At 19+4 weeks of gestation, the length of the cervix was measured to be 17 mm, (B) at 21+4 weeks of gestation, it was measured to be 7 mm and (C) after transabdominal cervicoisthmic cerclage it was measured to be 32 mm. (D) The photograph of the anterior side of the uterus after completion of transabdominal cervicoisthmic cerclage (case 2).
Reference
-
1. Zaveri V, Aghajafari F, Amankwah K, Hannah M. Abdominal versus vaginal cerclage after a failed transvaginal cerclage: a systematic review. Am J Obstet Gynecol. 2002; 187:868–872.2. Tulandi T, Alghanaim N, Hakeem G, Tan X. Pre and postconceptional abdominal cerclage by laparoscopy or laparotomy. J Minim Invasive Gynecol. 2014; 21:987–993.3. Ades A, Dobromilsky KC, Cheung KT, Umstad MP. Transabdominal cervical cerclage: laparoscopy versus laparotomy. J Minim Invasive Gynecol. 2015; 22:968–973.4. Pereira RM, Zanatta A, de Mello Bianchi PH, Yadid IM, da Motta EL, Serafini PC. Successful interval laparoscopic transabdominal cervicoisthmic cerclage preceding twin gestation: a case report. J Minim Invasive Gynecol. 2009; 16:634–638.5. Carter JF, Soper DE, Goetzl LM, Van Dorsten JP. Abdominal cerclage for the treatment of recurrent cervical insufficiency: laparoscopy or laparotomy? Am J Obstet Gynecol. 2009; 201:111.e1–111.e4.6. Shin SJ, Chung H, Kwon SH, Cha SD, Lee HJ, Kim AR, et al. The feasibility of a modified method of laparoscopic transabdominal cervicoisthmic cerclage during pregnancy. J Laparoendosc Adv Surg Tech A. 2015; 25:651–656.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful full-term delivery after abdominal radical trachelectomy and concurrent cervicoisthmic cerclage for early stage cervical cancer: Two cases
- A Case of Successful Spontaneous Pregnancy after Laparoscopic Radical Trachelectomy with Trans-Abdominal Cervicoisthmic Cerclage Treatment
- Two Case Review of Transvaginal Cervicoisthmic Cerclage
- Validity of Indications and Clinical Outcome of Transabdominal Cervicoisthmic Cerclage for Cervical Incompetence
- Study on Pregnancy Outcomes after Transabdominal Cervico-Isthmic Cerclage during Pregnancy
