J Lipid Atheroscler.
2016 Jun;5(1):37-47. 10.12997/jla.2016.5.1.37.
Long-term Clinical Outcomes in Acute Myocardial Infarction Patients with Left Ventricular Dysfunction
- Affiliations
-
- 1The Heart Center of Chonnam National University Hospital, Gwangju, Korea. myungho@chollian.net
- KMID: 2328837
- DOI: http://doi.org/10.12997/jla.2016.5.1.37
Abstract
OBJECTIVE
The purpose of this study was to define the effect of the changes of left ventricular ejection fraction (LVEF) on long-term major adverse cardiac events (MACEs) in patients with acute myocardial infarction (AMI).
METHODS
Clinical analysis was performed on 1,188 AMI patients who completed follow- up 2-dimensional (2D) echocardiography after one year and clinical follow-up for 5 years. These patients were divided into three groups according to the LVEF change ratio: group A [increased LVEF change ratio, N=626], group B [decreased LVEF change ratio<20%, N=414], group C [decreased LVEF change ratio≥20%, N=148].
RESULTS
Initial low LVEF group and normal LVEF group showed no differences in MACEs. The mean initial and follow-up LVEF were 54.4±12.2% and 60.4±12.3% in the group A, 54.6±13.0% and 47.9±12.1% in the group B, and 56.5±12.6% and 39.9±11.6% in the group C (p=0.71). Total MACEs occurred in 62 (9.9%) patients in the group A, 83 (20.0%) patients in the group B, 44 (29.7%) patients in the group C during 5-year clinical follow-up (p=0.01). Initial low EF (<45%) was not a risk factor for long-term MACEs (Odd ratio (OR), 1.686; 95% confidence index (CI), 0.861-2.862, p=0.065), but the LVEF change ratio was a strong risk factor for long-term MACEs (OR, 3.731; 95% CI, 2.039-6.828, p=0.001). MACE-free survivals of patients with initial low LVEF and patients with low LVEF during follow-up period showed no significant differences (p=0.731).
CONCLUSION
Initial low LVEF is not a predictor of long-term MACEs, but the decreased LVEF ratio during follow-up period is a strong predictor of long-term MACEs.
Keyword
MeSH Terms
Figure
-

Fig. 1 Major adverse cardiac event (MACE)-free survivals according to left ventricular ejection fraction (LVEF). (A) MACE-free survivals according to initial LVEF. Group I: initial LVEF <45%, Group II: initial LVEF ≥45%, (B) MACE-free survivals according to LVEF change. Group A: increased LVEF at follow-up compared with initial LVEF, Group B: decreased LVEF change ratio <20% at follow-up, Group C: patients with decreased LVEF change ratio ≥20% at follow-up.
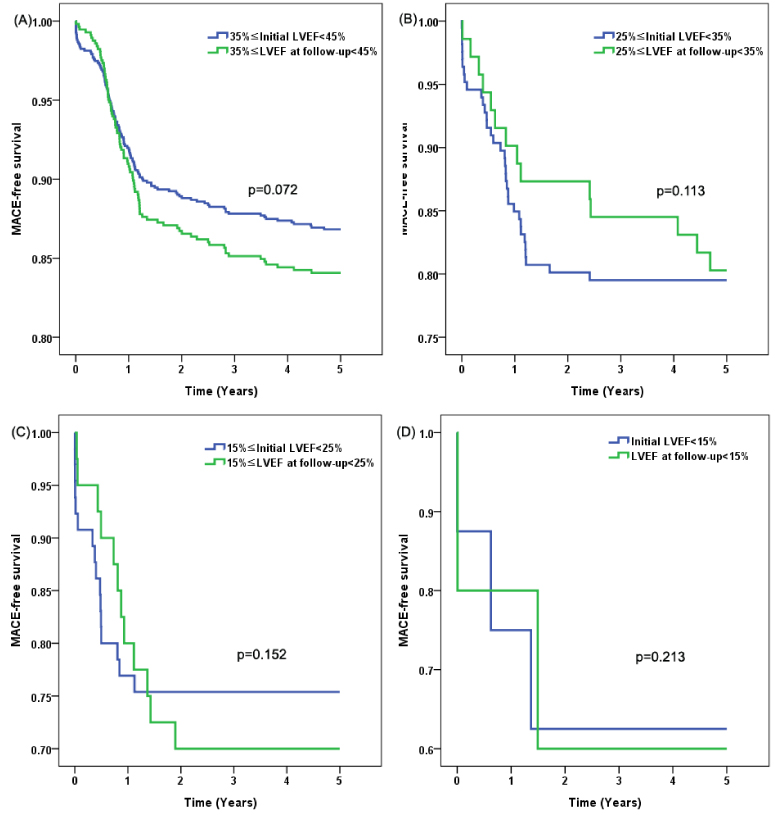
Fig. 2 Comparison of long-term MACEs between initial low LVEF and low LVEF at follow-up.
Reference
-
1. Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009; 119:e391–e479.2. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, et al. Heart disease and stroke statistics--2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009; 119:480–486.3. Lee DS, Austin PC, Rouleau JL, Liu PP, Naimark D, Tu JV. Predicting mortality among patients hospitalized for heart failure: derivation and validation of a clinical model. JAMA. 2003; 290:2581–2587.
Article4. Ambrosioni E, Borghi C, Magnani B. The Survival of Myocardial Infarction Long-Term Evaluation (SMILE) Study Investigators. The effect of the angiotensin-converting-enzyme inhibitor zofenopril on mortality and morbidity after anterior myocardial infarction. N Engl J Med. 1995; 332:80–85.
Article5. Bueno H, Vidán MT, Almazán A, López-Sendón JL, Delcán JL. Influence of sex on the short-term outcome of elderly patients with a first acute myocardial infarction. Circulation. 1995; 92:1133–1140.
Article6. Vasan RS, Larson MG, Benjamin EJ, Evans JC, Reiss CK, Levy D. Congestive heart failure in subjects with normal versus reduced left ventricular ejection fraction: prevalence and mortality in a population-based cohort. J Am Coll Cardiol. 1999; 33:1948–1955.
Article7. Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, et al. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American College of Chest Physicians and the International Society for Heart and Lung transplantation: endorsed by the Heart Rhythm Society. Circulation. 2005; 112:e154–e235.8. Sato Y, Nishi K, Taniguchi R, Miyamoto T, Fukuhara R, Yamane K, et al. In patients with heart failure and non-ischemic heart disease, cardiac troponin T is a reliable predictor of long-term echocardiographic changes and adverse cardiac events. J Cardiol. 2009; 54:221–230.
Article9. Buckley DI, Fu R, Freeman M, Rogers K, Helfand M. C-reactive protein as a risk factor for coronary heart disease: a systematic review and meta-analyses for the U.S. Preventive Services Task Force. Ann Intern Med. 2009; 151:483–495.
Article10. Jafary FH. Devereux formula for left ventricular mass--be careful to use the right units of measurement. J Am Soc Echocardiogr. 2007; 20:783.
Article11. Solomon SD, Anavekar N, Skali H, McMurray JJ, Swedberg K, Yusuf S, et al. Influence of ejection fraction on cardiovascular outcomes in a broad spectrum of heart failure patients. Circulation. 2005; 112:3738–3744.
Article12. Mentz RJ, Fiuzat M, Shaw LK, Phillips HR, Borges-Neto S, Felker GM, et al. Comparison of clinical characteristics and long-term outcomes of patients with ischemic cardiomyopathy with versus without angina pectoris (from the Duke Databank for Cardiovascular Disease). Am J Cardiol. 2012; 109:1272–1277.
Article13. Fang J, Mensah GA, Croft JB, Keenan NL. Heart failure-related hospitalization in the U.S., 1979 to 2004. J Am Coll Cardiol. 2008; 52:428–434.
Article14. Parkash R, Maisel WH, Toca FM, Stevenson WG. Atrial fibrillation in heart failure: high mortality risk even if ventricular function is preserved. Am Heart J. 2005; 150:701–706.
Article15. Shahar E, Lee S, Kim J, Duval S, Barber C, Luepker RV. Hospitalized heart failure: rates and long-term mortality. J Card Fail. 2004; 10:374–379.
Article16. Pocock SJ, Wang D, Pfeffer MA, Yusuf S, McMurray JJ, Swedberg KB, et al. Predictors of mortality and morbidity in patients with chronic heart failure. Eur Heart J. 2006; 27:65–75.
Article17. Drazner MH, Rame JE, Marino EK, Gottdiener JS, Kitzman DW, Gardin JM, et al. Increased left ventricular mass is a risk factor for the development of a depressed left ventricular ejection fraction within five years: the Cardiovascular Health Study. J Am Coll Cardiol. 2004; 43:2207–2215.
Article18. Gottdiener JS, Arnold AM, Aurigemma GP, Polak JF, Tracy RP, Kitzman DW, et al. Predictors of congestive heart failure in the elderly: the Cardiovascular Health Study. J Am Coll Cardiol. 2000; 35:1628–1637.
Article19. Udelson JE. Heart failure with preserved ejection fraction. Circulation. 2011; 124:e540–e543.
Article20. Borlaug BA, Paulus WJ. Heart failure with preserved ejection fraction: pathophysiology, diagnosis, and treatment. Eur Heart J. 2011; 32:670–679.
Article21. Dohadwala M, Estes NA 3rd, Link MS. New paradigms in the prevention of sudden cardiac arrest and heart failure treatment. Curr Cardiol Rep. 2011; 13:377–386.
Article22. Kinjo K, Sato H, Sato H, Ohnishi Y, Hishida E, Nakatani D, et al. Prognostic significance of atrial fibrillation/atrial flutter in patients with acute myocardial infarction treated with percutaneous coronary intervention. Am J Cardiol. 2003; 92:1150–1154.
Article23. Crenshaw BS, Ward SR, Granger CB, Stebbins AL, Topol EJ, Califf RM. Atrial fibrillation in the setting of acute myocardial infarction: the GUSTO-I experience. Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries. J Am Coll Cardiol. 1997; 30:406–413.
Article24. Beukema RJ, Elvan A, Ottervanger JP, de Boer MJ, Hoorntje JC, Suryapranata H, et al. Atrial fibrillation after but not before primary angioplasty for ST-segment elevation myocardial infarction of prognostic importance. Neth Heart J. 2012; 20:155–160.
Article25. Goldberg A, Hammerman H, Petcherski S, Zdorovyak A, Yalonetsky S, Kapeliovich M, et al. Inhospital and 1-year mortality of patients who develop worsening renal function following acute ST-elevation myocardial infarction. Am Heart J. 2005; 150:330–337.
Article26. Rodrigues FB, Bruetto RG, Torres US, Otaviano AP, Zanetta DM, Burdmann EA. Effect of kidney disease on acute coronary syndrome. Clin J Am Soc Nephrol. 2010; 5:1530–1536.
Article27. Rihal CS, Textor SC, Grill DE, Berger PB, Ting HH, Best PJ, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002; 105:2259–2264.
Article28. Devereux RB, de Simone G, Ganau A, Roman MJ. Left ventricular hypertrophy and geometric remodeling in hypertension: stimuli, functional consequences and prognostic implications. J Hypertens Suppl. 1994; 12:S117–S127.29. Muiesan ML, Salvetti M, Monteduro C, Bonzi B, Paini A, Viola S, et al. Left ventricular concentric geometry during treatment adversely affects cardiovascular prognosis in hypertensive patients. Hypertension. 2004; 43:731–738.
Article30. Drazner MH. The progression of hypertensive heart disease. Circulation. 2011; 123:327–334.
Article31. Rosen BD, Fernandes VR, Nasir K, Helle-Valle T, Jerosch-Herold M, Bluemke DA, et al. Age, increased left ventricular mass, and lower regional myocardial perfusion are related to greater extent of myocardial dyssynchrony in asymptomatic individuals: the multiethnic study of atherosclerosis. Circulation. 2009; 120:859–866.
Article32. Lonn E, Shaikholeslami R, Yi Q, Bosch J, Sullivan B, Tanser P, et al. Effects of ramipril on left ventricular mass and function in cardiovascular patients with controlled blood pressure and with preserved left ventricular ejection fraction: a substudy of the Heart Outcomes Prevention Evaluation (HOPE) Trial. J Am Coll Cardiol. 2004; 43:2200–2206.
Article33. Fak AS, Okucu M, Tezcan H, Bodur G, Oktay A. The effects of amlodipine on left ventricular mass and diastolic function in concentric and eccentric left ventricular hypertrophy. J Cardiovasc Pharmacol Ther. 1996; 1:95–100.
Article34. Edwards NC, Steeds RP, Stewart PM, Ferro CJ, Townend JN. Effect of spironolactone on left ventricular mass and aortic stiffness in early-stage chronic kidney disease: a randomized controlled trial. J Am Coll Cardiol. 2009; 54:505–512.
Article35. Lee TM, Lin MS, Chou TF, Tsai CH, Chang NC. Effects of pravastatin on left ventricular mass in patients with hyperlipidemia and essential hypertension. Atherosclerosis. 2004; 176:273–278.
Article36. Su SF, Hsiao CL, Chu CW, Lee BC, Lee TM. Effects of pravastatin on left ventricular mass in patients with hyperlipidemia and essential hypertension. Am J Cardiol. 2000; 86:514–518.
Article37. Bloch Thomsen PE, Jons C, Raatikainen MJ, Moerch Joergensen R, Hartikainen J, Virtanen V, et al. Long-term recording of cardiac arrhythmias with an implantable cardiac monitor in patients with reduced ejection fraction after acute myocardial infarction: the cardiac arrhythmias and risk stratification after acute myocardial infarction (CARISMA) study. Circulation. 2010; 122:1258–1264.
Article38. Richards AM, Nicholls MG, Espiner EA, Lainchbury JG, Troughton RW, Elliott J, et al. B-type natriuretic peptides and ejection fraction for prognosis after myocardial infarction. Circulation. 2003; 107:2786–2792.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ventricular Extrasystoles in Convalescent Phase of Acute Myocardial Infarction
- Impact of ST segment deviation in patients with acute myocardial infarction and left ventricular systolic dysfunction
- Incidence of Left Ventricular Thrombus after Acute Myocardial Infarction
- Assessment of Left and Right Ventricular Performance by Gated Blood Pool Scan in Acute Transmural Myocardial Infarction
- Assessment of Myocardial Viability Using PET
