Risk of Encountering Dorsal Scapular and Long Thoracic Nerves during Ultrasound-guided Interscalene Brachial Plexus Block with Nerve Stimulator
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Wonkwang University College of Medicine, Wonkwang Institute of Science, Iksan, Korea.
- 2Department of Anesthesiology and Pain Medicine, Presbyterian Medical Center, University of Seonam College of Medicine, Jeonju, Korea. ingwei2475@naver.com
- KMID: 2327639
- DOI: http://doi.org/10.3344/kjp.2016.29.3.179
Abstract
- BACKGROUND
Recently, ultrasound has been commonly used. Ultrasound-guided interscalene brachial plexus block (IBPB) by posterior approach is more commonly used because anterior approach has been reported to have the risk of phrenic nerve injury. However, posterior approach also has the risk of causing nerve injury because there are risks of encountering dorsal scapular nerve (DSN) and long thoracic nerve (LTN). Therefore, the aim of this study was to evaluate the risk of encountering DSN and LTN during ultrasound-guided IBPB by posterior approach.
METHODS
A total of 70 patients who were scheduled for shoulder surgery were enrolled in this study. After deciding insertion site with ultrasound, awake ultrasound-guided IBPB with nerve stimulator by posterior approach was performed. Incidence of muscle twitches (rhomboids, levator scapulae, and serratus anterior muscles) and current intensity immediately before muscle twitches disappeared were recorded.
RESULTS
Of the total 70 cases, DSN was encountered in 44 cases (62.8%) and LTN was encountered in 15 cases (21.4%). Both nerves were encountered in 10 cases (14.3%). Neither was encountered in 21 cases (30.4%). The average current measured immediately before the disappearance of muscle twitches was 0.44 mA and 0.50 mA at DSN and LTN, respectively.
CONCLUSIONS
Physicians should be cautious on the risk of injury related to the anatomical structures of nerves, including DSN and LTN, during ultrasound-guided IBPB by posterior approach. Nerve stimulator could be another option for a safer intervention. Moreover, if there is a motor response, it is recommended to select another way to secure better safety.
Keyword
MeSH Terms
Figure
-
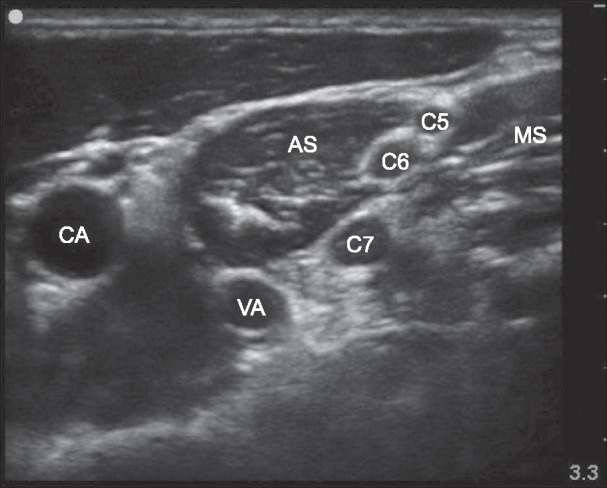
Fig. 1 Ultrasound image of the site of interscalene brachial plexus block. CA: carotid artery, VA: vertebral artery, AS: anterior scalene muscle, MS: middle scalene muscle, C5: 5th cervical root, C6: 6th cervical root, C7: 7th cervical root.
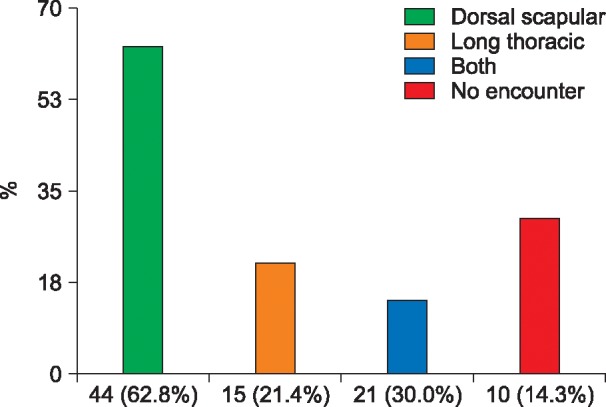
Fig. 2 Risk of encountering dorsal scapular nerve and long thoracic nerve.
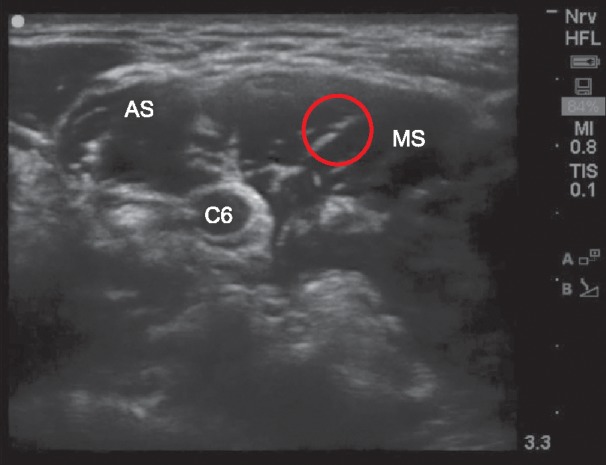
Fig. 3 Ultrasound image of dorsal scapular nerve. It derives from C5 nerve root. AS: anterior scalene muscle, MS: middle scalene muscle, Red circle: dorsal scapular nerve, C6: 6th cervical root.
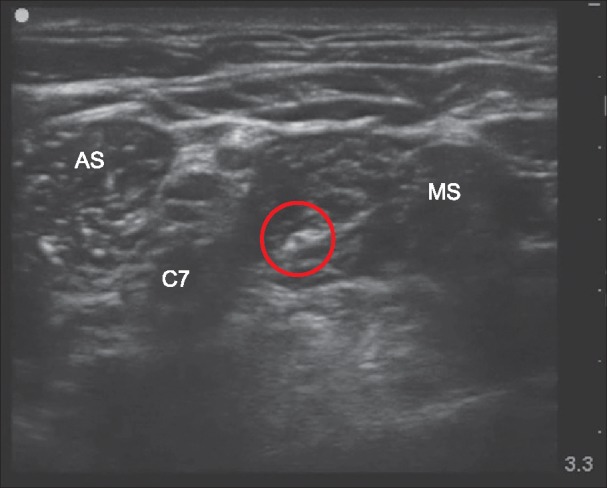
Fig. 4 Ultrasound image of long thoracic nerve. It arises from the anterior branches of the 6th cervical nerve root. AS: anterior scalene muscle, MS: middle scalene muscle, Red circle: long thoracic nerve, C7: 7th cervical root.
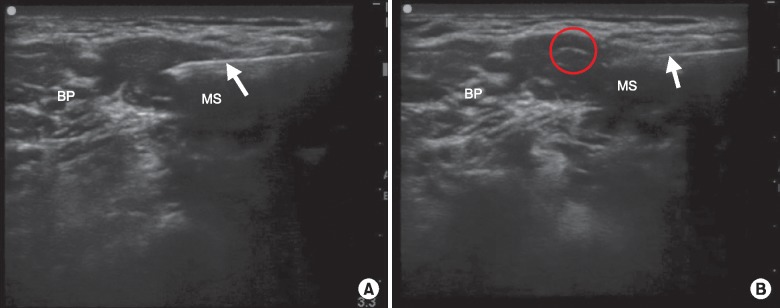
Fig. 5 Ultrasound image of dual-guided interscalene brachial plexus block (A) and just cephalad image of A (B). Dorsal scapular nerve and long thoracic nerve are not seen (A). Dorsal scapular nerve is seen. It already passed and went to the cephalad direction of needle path (B). BP: brachial plexus, MS: middle scalene muscle, Red circle: dorsal scapular nerve, Arrow: needle.
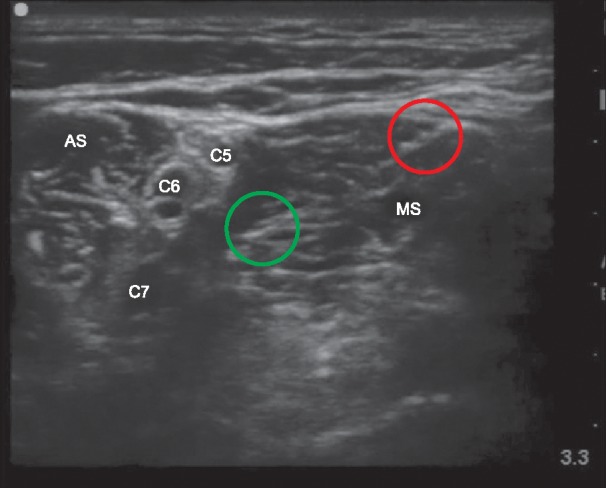
Fig. 6 Ultrasound image of dorsal scapular nerve and long thoracic nerve at the site of interscalene brachial plexus block. Dorsal scapular nerve and long thoracic nerve are seen in the middle scalene muscle. AS: anterior scalene muscle, MS: middle scalene muscle, Red circle: dorsal scapular nerve, Green circle: long thoracic nerve, C5: 5th cervical root, C6: 6th cervical root, C7: 7th cervical root.
Cited by 4 articles
-
Optimal Cut-Off Value of the Coracohumeral Ligament Area as a Morphological Parameter to Confirm Frozen Shoulder
Hyung Rae Cho, Byong Hyon Cho, Keum Nae Kang, Young Uk Kim
J Korean Med Sci. 2020;35(15):e99. doi: 10.3346/jkms.2020.35.e99.New insights into pathways of the dorsal scapular nerve and artery for selective dorsal scapular nerve blockade
Hyunho Cho, Seungwoo Kang, Hyung-Sun Won, Miyoung Yang, Yeon-Dong Kim
Korean J Pain. 2019;32(4):307-312. doi: 10.3344/kjp.2019.32.4.307.A pictorial review of signature patterns living in musculoskeletal ultrasonography
Su Young Kim, Ji Hyun Cheon, Won Jun Seo, Geun Young Yang, Yun Mi Choi, Kyung Hoon Kim
Korean J Pain. 2016;29(4):217-228. doi: 10.3344/kjp.2016.29.4.217.Recent updates on interscalene brachial plexus block for shoulder surgery
RyungA Kang, Justin Sangwook Ko
Anesth Pain Med. 2023;18(1):5-10. doi: 10.17085/apm.22254.
Reference
-
1. Kessler J, Schafhalter-Zoppoth I, Gray AT. An ultrasound study of the phrenic nerve in the posterior cervical triangle: implications for the interscalene brachial plexus block. Reg Anesth Pain Med. 2008; 33:545–550. PMID: 19258969.
Article2. Kim HJ, Park SH, Shin HY, Choi YS. Brachial plexus injury as a complication after nerve block or vessel puncture. Korean J Pain. 2014; 27:210–218. PMID: 25031806.
Article3. Lee LA, Domino KB. Complications associated with peripheral nerve blocks: lessons from the ASA closed claims project. Int Anesthesiol Clin. 2005; 43:111–118. PMID: 15970748.
Article4. Kim YD, Moon HS. Review of medical dispute cases in the pain management in Korea: a medical malpractice liability insurance database study. Korean J Pain. 2015; 28:254–264. PMID: 26495080.
Article5. Mian A, Chaudhry I, Huang R, Rizk E, Tubbs RS, Loukas M. Brachial plexus anesthesia: a review of the relevant anatomy, complications, and anatomical variations. Clin Anat. 2014; 27:210–221. PMID: 23959836.
Article6. Jenkins GW, Kemnitz CP, Tortora GJ. Anatomy and physiology: from science to life. Hoboken (NJ): John Wiley & Sons;2007.7. Tubbs RS, Tyler-Kabara EC, Aikens AC, Martin JP, Weed LL, Salter EG, et al. Surgical anatomy of the dorsal scapular nerve. J Neurosurg. 2005; 102:910–911. PMID: 15926718.
Article8. Saporito A. Dorsal scapular nerve injury: a complication of ultrasound-guided interscalene block. Br J Anaesth. 2013; 111:840–841. PMID: 24108729.
Article9. Horwitz MT, Tocantins LM. An anatomical study of the role of the long thoracic nerve and the related scapular bursae in the pathogenesis of local paralysis of the serratus anterior muscle. Anat Rec. 1938; 71:375–385.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound Guided Low Approach Interscalene Brachial Plexus Block for Upper Limb Surgery
- Bilateral variant locations of the musculocutaneous nerve during ultrasound-guided bilateral axillary brachial plexus block: A case report
- Variations of the ventral rami of the brachial plexus
- Prolonged Horner's Syndrome Following Interscalene Brachial Plexus Block: A case report
- Phrenic Nerve Paralysis following Interscalene Bracheal Plexus Block
