Precise Muscle Selection Using Dynamic Polyelectromyography for Treatment of Post-stroke Dystonia: A Case Report
- Affiliations
-
- 1Department of Rehabilitation Medicine and Research Institute of Rehabilitation Medicine, Yonsei University College of Medicine, Seoul, Korea.
- 2Department of Neurology, Yonsei University College of Medicine, Seoul, Korea.
- 3Department of Physical Medicine and Rehabilitation, Veterans Health Service Medical Center, Seoul, Korea.
- KMID: 2327620
- DOI: http://doi.org/10.5535/arm.2016.40.3.551
Abstract
- Dystonia has a wide range of causes, but treatment of dystonia is limited to minimizing the symptoms as there is yet no successful treatment for its cause. One of the optimal treatment methods for dystonia is chemodenervation using botulinum toxin type A (BTX-A), alcohol injection, etc., but its success depends on how precisely the dystonic muscle is selected. Here, we reported a successful experience in a 49-year-old post-stroke female patient who showed paroxysmal repetitive contractions involving the right leg, which may be of dystonic nature. BTX-A and alcohol were injected into the muscles which were identified by dynamic polyelectromyography. After injection, the dystonic muscle spasm, cramping pain, and the range of motion of the affected lower limb improved markedly, and she was able to walk independently indoors. In such a case, dynamic polyelectromyography may be a useful method for selecting the dominant dystonic muscles.
Keyword
MeSH Terms
Figure
-
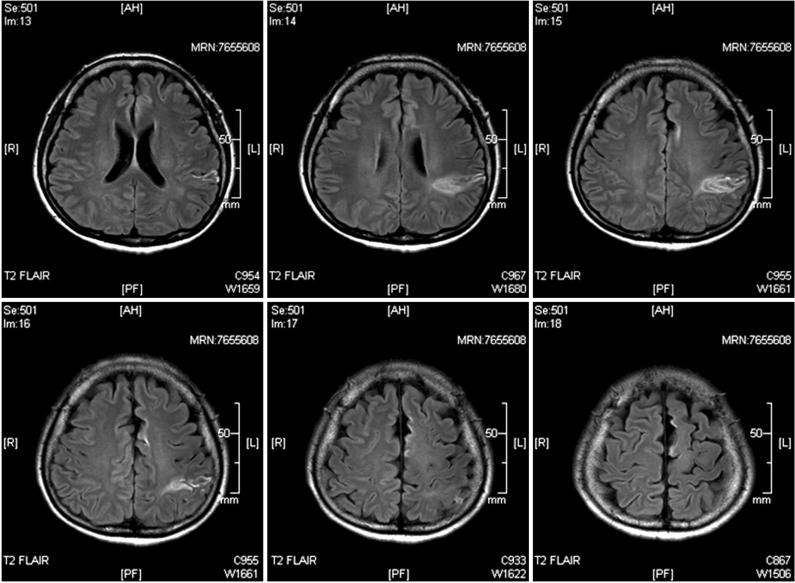
Fig. 1 Brain magnetic resonance imaging showed left middle cerebral artery infarction, involving the frontal and parietal lobes.

Fig. 2 Using the 10-channel electromyography mode, dynamic polyelectromyography was performed during the dystonic event. Motor unit action potentials of each lower extremity were recorded simultaneously.
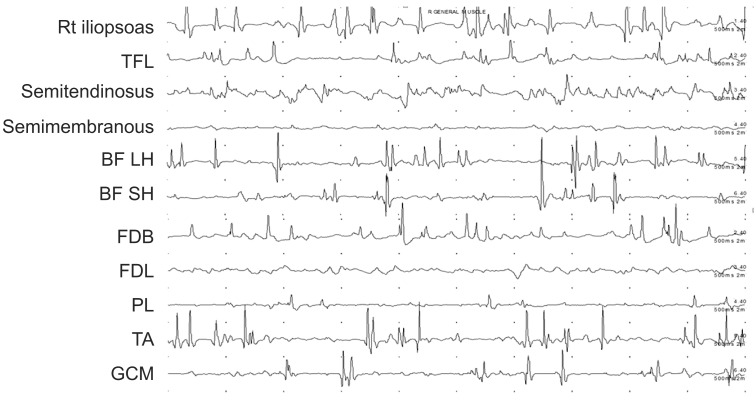
Fig. 3 Findings of dynamic polyelectromyography in the affected lower limb muscles at baseline. TFL, tensor fascia lata; BF LH, biceps femoris long head; BF SH, biceps femoris short head; FDB, flexor digitorum brevis; FDL, flexor digitorum longus; PL, peroneus longus; TA, tibialis anterior; GCM, gastrocnemius.

Fig. 4 Changes in the affected lower limb on a lateral view before injection (A); the knee flexor could not be extended by hand almost all day. (B) After injection, her knee could be extended to a near normal range.
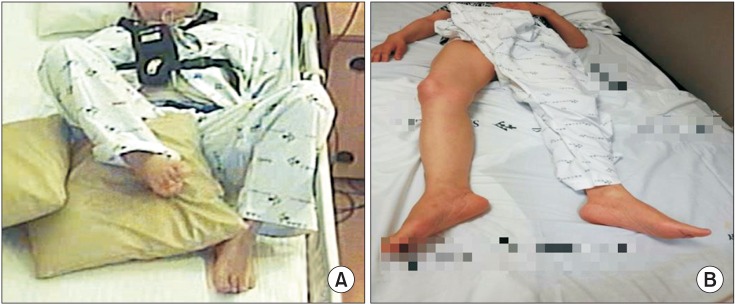
Fig. 5 Changes in the affected lower limb on a superior view before injection (A); her right hip and knee flexor were hyperactive with severe muscle cramping pain. (B) After injection, the flexed posture and pain were remarkably decreased.
Reference
-
1. Fahn S. Concept and classification of dystonia. Adv Neurol. 1988; 50:1–8. PMID: 3041755.2. Alarcon F, Zijlmans JC, Duenas G, Cevallos N. Poststroke movement disorders: report of 56 patients. J Neurol Neurosurg Psychiatry. 2004; 75:1568–1574. PMID: 15489389.
Article3. Jankovic J. Treatment of cervical dystonia with botulinum toxin. Mov Disord. 2004; 19(Suppl 8):S109–S115. PMID: 15027062.
Article4. Nijmeijer SW, Koelman JH, Kamphuis DJ, Tijssen MA. Muscle selection for treatment of cervical dystonia with botulinum toxin: a systematic review. Parkinsonism Relat Disord. 2012; 18:731–736. PMID: 22575237.5. Esquenazi A, Cioni M, Mayer NH. Assessment of muscle overactivity and spasticity with dynamic polyelectromyography and motion analysis. Open Rehabil J. 2010; 3:143–148.
Article6. Steeves TD, Day L, Dykeman J, Jette N, Pringsheim T. The prevalence of primary dystonia: a systematic review and meta-analysis. Mov Disord. 2012; 27:1789–1796. PMID: 23114997.
Article7. Takeuchi N, Chuma T, Mano Y. Phenol block for cervical dystonia: effects and side effects. Arch Phys Med Rehabil. 2004; 85:1117–1120. PMID: 15241760.
Article8. Jankovic J. Medical treatment of dystonia. Mov Disord. 2013; 28:1001–1012. PMID: 23893456.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Improvement of Lingual Dystonia Following Cerebellar Infarction through Botulinum Toxin Injection: a Case Report
- Botulinum Toxin Injection Therapy for Lingual Dystonia: A Case Report
- Delayed-onset focal dystonia after stroke
- A Case of Clozapine Treatment for Tardive Dystonia in Chronic Schizophrenia
- Verification of the Dystonic Muscles Using 18F-Fluorodeoxyglucose Positron Emission Tomography in a Patient with Cervical Dystonia: A case report
