J Korean Soc Spine Surg.
2005 Dec;12(4):275-280.
The Comparison of Rigid and Semi-rigid Rod for the Correctability of the Thoracic Hypokyphosis of the Idiopathic Scoliosis
- Affiliations
-
- 1Spine Centery, Centum Hospital, Pusan, Korea. ahnsjosdept@lycos.co.kr
- 2Department of Orthopedic Surgery, Daedong Hospital, Pusan, Korea.
Abstract
- STUDY DESIGN: The analysis was based on the sagittal and coronal correction of 64 cases of thoracic hyphokyphosis that were due to idiopathic scoliosis.
PURPOSE: We wanted to compare the three pedicle screws and rod systems (using either a semirigid and rigid rod) from the view points of the coronal and sagittal plane correction during the surgical treatment of idiopathic scoliosis.
SUMMARY OF LITERATURE REVIEW: There haven't been any reports that have compared the differences and their significance between the semirigid and rigid rod systems for correcting the thoracic hypokyphosis of idiopathic scoliosis.
MATERIALS AND METHODS
After a minimum follow-up of 1 year, the results of the frontal and sagittal correction of each study group were compared. There were a total of 52 females and 12 males. The mean age at the time of surgical intervention was 16.4 (age range: 12~24). CD instrumentation with a rigid stainless steel rod (7 mm in diameter and 1200 N/mm for its stiffness) was used in group I (36 patients), and 4-CI instrumentation with a titanium alloy rod (6.35 mm in diameter and 1200 N/mm for its stiffness) was used in group II (18 patients). Xia instrumentation with a semi-rigid rod (6 mm in diameter and 600 N/mm for its stiffness) was used in group III (10 patients). For all patients undergoing the segmental pedicle screw fixation procedure, pedicle screws were inserted into every vertebra on the concave side, in the end of each vertebra and then alternately in every other vertebra on the convex side. We measured the preoperative and postoperative magnitude of the major and compensatory curves, the thoracic kyphotic angle on the standing radiographs and the flexibility of the curve. We statistically compared the correctability of thoracic kyphotic angle between the rigid and semi-rigid rods.
RESULTS
The differences of preoperative and postoperative major curves in groups I, II and III were 47.3 degrees/12.7 degrees, 51.6 degrees/12.3 degrees and 49.6 degrees/13.3 degrees respectively. The thoracic kyphotic angle was 22.6 degrees/26.6 degrees, 22.0 degrees/26.9 degrees and 23.8 degrees/22.8 degrees, respectively. There was no significant difference for the correction of the coronal angle in each group, but groups I and II were superior to group III for the rate of correcting the kyphotic angle.
CONCLUSION
The rod should be stiff enough to pull the spine posteromedially when using the derotation technique for the surgical treatment of idiopathic scoliosis.
Keyword
MeSH Terms
Figure
-

Fig. 1. (A) In group I (CD instrumentation), Preoperative major thoracic curve was 59° and kyphotic angle was 8°. (B) In the fifth postoperative year, Major curve was corrected to 21° and thoracic kyphosis was improved from 8° to 19°.

Fig. 2. (A) In group II(4-CIS instrumentation), Double thoracic curve was 37° & 50°, thoracic kyphosis was 33°. (B) In the second postoperative year, major curve was corrected to 20°, 18° and thoracic kyphosis was improved from 33° to 36°.
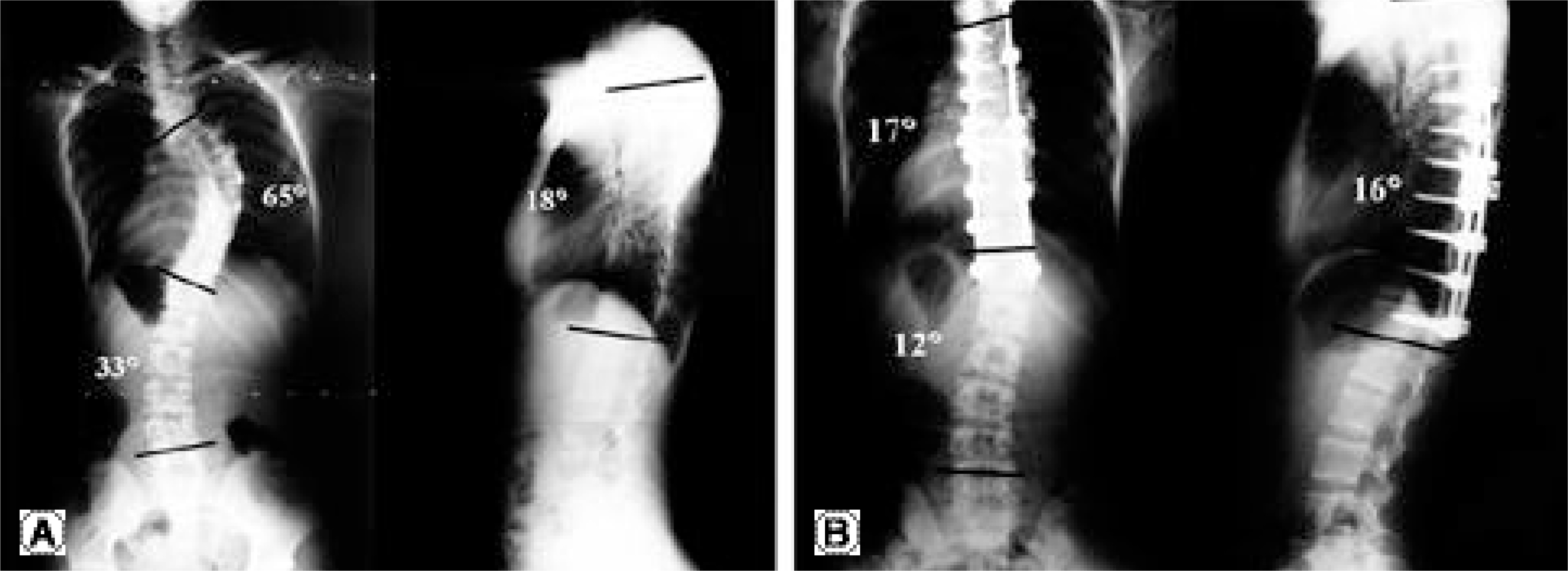
Fig. 3. (A) In group III (XIA instrumentation), Preoperative major thoracic curve was 65° and kyphotic angle was 18°. (B) In the second postoperative year, major curve was corrected to 17° but thoracic kyphosis worsened from 18° to 16°.
Reference
-
1). Bergofsky EH. Respiratory failure in disorders of the thoracic cage. Am Rev Respir Dis. 119:643–669. 1979.2). Bjure J, Grimby G, Kasaliku J, Lindh M and Nachemson A. Respiratory impairment and airway closure in patients with untreated idiopathic scoliosis. Thorax. 25:451–456. 1970.
Article3). Bradford DS, Blatt JM and Rasp FL. Surgical management of severe thoracic lordosis. A new technique to restore normal kyphosis. Spine. 8:420–8. 1983.4). Caro CG and Cubis AB. Pulmonary function in kyphoscoliosis. Thorax. 16:282–290. 1961.
Article5). Cotrel Y, Dubousset J and Guillaumat M. New universal instrumentation in spinal surgery. Clin Orthop. 227:10–23. 1988.
Article6). Harrinton PR. Treatment of scoliosis. J Bone Joint Surg. 44-A:591–610. 1962.7). Levine DB. Pulmonary function in scoliosis. Orthop Clin North Am. 10:761–768. 1979.
Article8). McMaster MJ. Luque rod instrumentation in the treatment of adolescent idiopathic scoliosis. J Bone Joint Surg. 73-B:982–989. 1991.
Article9). Muschik M, Schlenzka D, Robinson PN, et al. D orsal instrumentation for idiopathic adolescent thoracic scoilo -sis. Eur Spine J. 8:93–9. 1999.10). Nash CL and Moe JH. A study of vertebral rotation. J Bone Joint Surg. 51-A:223–229. 1969.11). Nash CL and Nevins K. A lateral look at pulmonary function in scoliosis in proceedings of the Scoliosis Research Society. J Bone Joint Surg. 55-A:440. 1974.12). Suk SI, Lee CK and Chung SS. Comparison of Zielke ventral derotation system and Cotrel-Dubousset instrumentation in the treatment of idiopathic lumbar and thoracolumbar scoliosis. Spine. 19:419–29. 1994.
Article13). Suk SI, Lee CK, Kim WJ, et al. Segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis. Spine. 20:1399–405. 1995.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Severe Rigid Scoliosis: Review of Management Strategies and Role of Spinal Osteotomies
- Segmental pedicle screw fixation in the treatment of Thoracic idiopathic scoliosis
- Pedicle Screw Instrumentation for Adolescent Idiopathic Scoliosis: The Insertion Technique, the Fusion Levels and Direct Vertebral Rotation
- Scoliosis Associated with Marfan Syndrome
- Segmental Spinal Instrumentation in the Treatment of Scoliosis
