Clusters of oral health-related behaviors by gender and their relationship with psychosocial factors for adolescents in Gangneung
- Affiliations
-
- 1Department of Preventive and Public Health Dentistry, Research Institute of Oral Science, Gangneung-Wonju National University College of Dentistry, Gangneung, Korea. feeljsh@gwnu.ac.kr
Abstract
OBJECTIVES
To verify the clusters of oral health-related behaviors by gender for adolescents in Gangneung, and to assess the influences of psychosocial factors (family socioeconomic status factors, individual economic factors, and psychological factors) on these clusters.
METHODS
A survey was conducted of 3,611 adolescents (6th grade students in primary school, 2nd grade students in middle school, and 2nd grade students in high school) in Gangneung. The response rate was 96.6% (1,846 boys; 1,765 girls). The data were collected via self-administered structured questionnaires assessing participants 'smoking experience,' 'tooth brushing,' 'consumption of crackers or soft drinks,' and 'consumption of fruits or vegetables.' K-means cluster analysis was used to cluster the oral health-related behaviors by gender. A chi-square test was used to assess the difference between the clusters for oral health-related behaviors by gender and psychosocial factors.
RESULTS
Clusters of oral health related-behaviors were classified into the unhealthy group (group 1; bad oral health-related behaviors), healthy group (group 2; good behaviors), and complex group (group 3; low smoking experiences and complex other behaviors). The clusters were different by gender. In the unhealthy group, boys represented 19.9% while, in the healthy group, girls represented 47.3%, which are both higher than the theoretical rates. Psychosocial factors in the unhealthy group were significantly lower than the healthy group (P<0.05).
CONCLUSIONS
Meaningful clusters of oral health-related behaviors by gender were identified. Furthermore, the clusters were different by psychosocial factors. This finding suggests that one of the best ways to enhance oral health for adolescents is to develop oral health promotion programs for each oral health-related behavior cluster.
Keyword
MeSH Terms
Figure
-
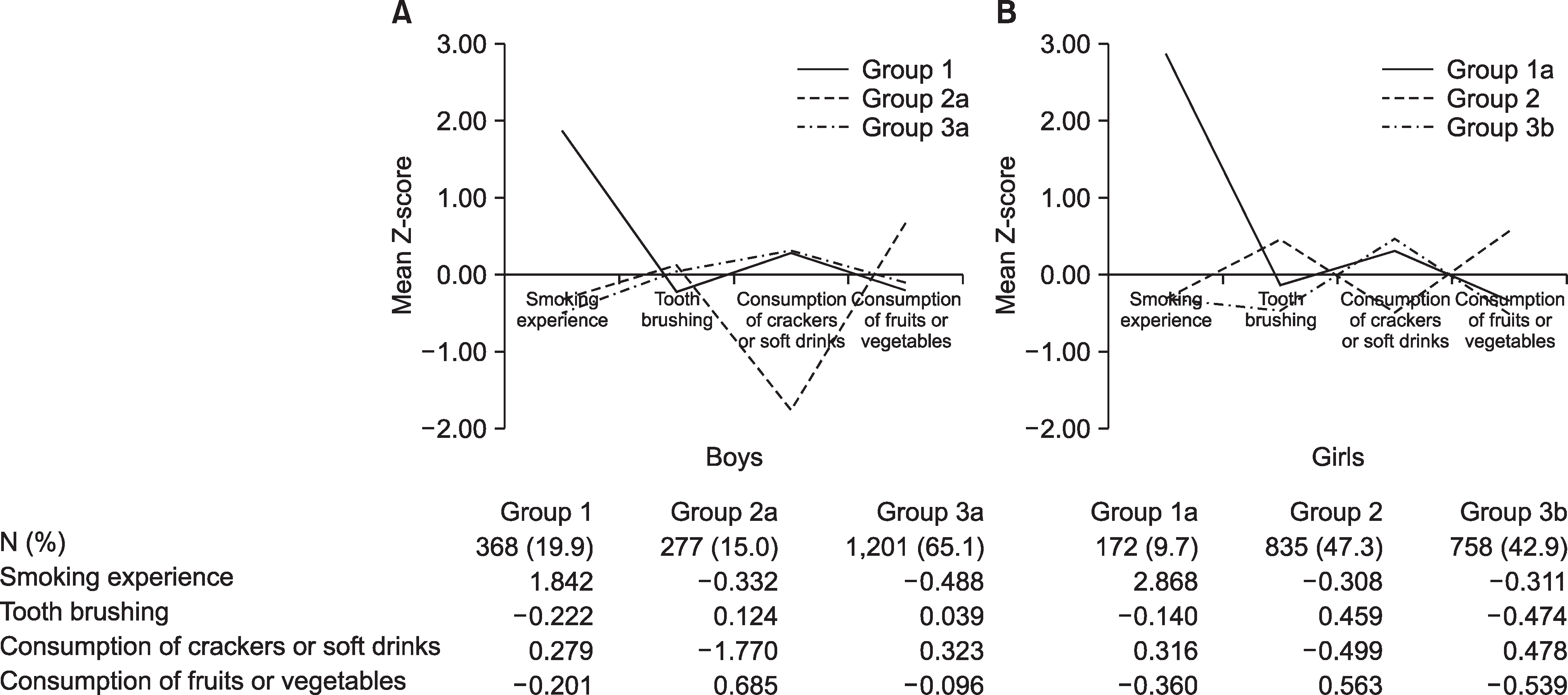
Fig. 1. Oral health related behaviors clusters by gender. *Final cluster centres in Z-score. Group 1 (unhealthy cluster): high smoking experience, low tooth brushing, high consumption of crackers or soft drinks, low consumption of fruits or vegetables. Group 1a: high smoking experience, high consumption of crackers or soft drinks, low consumption of fruits or vegetables. Group 2 (healthy cluster): low smoking experience, high tooth brushing, low consumption of crackers or soft drinks, high consumption of fruits or vegetables. Group 2a: low smoking experience, low consumption of crackers or soft drinks, high consumption of fruits or vegetables. Group 3 (complex cluster). Group 3a: low smoking experience, high consumption of crackers or soft drinks. Group 3b: low smoking experience, low tooth brushing, high consumption of crackers or soft drinks, low consumption of fruits or vegetables.
Reference
-
References
1. Bartlett R, Holditch-Davis D, Belyea M. Clusters of problem behaviors in adolescents. Res Nurs Health. 2005; 28:230–239.
Article2. Burke V, Milligan RA, Beilin LJ, Dunbar D, Spencer M, Balde E, et al. Clustering of health-related behaviors among 18-year-old Australians. Prev Med. 1997; 26:724–733.
Article3. de Vries H, van’t Riet J, Spigt M, Metsemakers J, van den Akker M, Vermunt JK, et al. Clusters of lifestyle behaviors: Results from the dutch SMILE study. Prev Med. 2008; 46:203–208.
Article4. Faeh D, Viswanathan B, Chiolero A, Warren W, Bovet P. Clustering of smoking, alcohol drinking and cannabis use in adolescents in a rapidly developing country. BMC Public Health. 2006; 6:169.
Article5. Kim JH. Youth health risk behavior survey in Korea [master’s thesis]. Seoul: Hanyang Univ.;2004. [Korean].6. Alamian A, Paradis G. Clustering of chronic disease behavioral risk factors in Canadian children and adolescents. Prev Med. 2009; 48:493–499.
Article7. Shin SJ, Ahn YS, Jung SH. The relationship between dental health behaviors and socioeconomic status among Korean adolescents. J Korean Acad Oral Health. 2008; 32:223–230.8. Jackson C, Sweeting H, Haw S. Clustering of substance use and sexual risk behaviour in adolescence: Analysis of two cohort studies. BMJ Open. 2012; 2:e000661.
Article9. Friestad C, Klepp KI. Socioeconomic status and health behaviour patterns through adolescence: Results from a prospective cohort study in Norway. Eur J Public Health. 2006; 16:41–47.
Article10. Cutler GJ, Flood A, Hannan P, Neumark-Sztainer D. Multiple sociodemographic and socioenvironmental characteristics are correlated with major patterns of dietary intake in adolescents. J Am Diet Assoc. 2011; 111:230–240.
Article11. Kang HS. Relationships between dietary behaviors and oral health behaviors of middle school students in Gyeonggi area [master’s thesis]. Seoul: Myongji Univ.;2012. [Korean].12. Zaborskis A, Lagunaite R, Busha R, Lubiene J. Trend in eating habits among Lithuanian school-aged children in context of social inequality: Three cross-sectional surveys 2002, 2006 and 2010. BMC Public Health. 2012; 12:52.
Article13. Ottevaere C, Huybrechts I, Benser J, De Bourdeaudhuij I, Cuen-ca-Garcia M, Dallongeville J, et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Health. 2011; 11:328.
Article14. Conry MC, Morgan K, Curry P, McGee H, Harrington J, Ward M, et al. The clustering of health behaviours in Ireland and their relationship with mental health, self-rated health and quality of life. BMC Public Health. 2011; 11:692.
Article15. Sheiham A, Bonecker M. Promoting children’s oral health theory & practice. UK: Quintessence;2006. p. 7–8.16. Daly B, Watt R, Batchelor P, Treasure E. Essential dental public health. UK: Oxford Univ press;2002. p. 353.17. Jung SH, Tsakos G, Sheiham A, Ryu JI, Watt RG. Socio-economic status and oral health-related behaviours in Korean adolescents. Soc Sci Med. 2010; 70:1780–1788.
Article18. Levin KA, Currie C. Adolescent toothbrushing and the home environment: Sociodemographic factors, family relationships and mealtime routines and disorganisation. Community Dent Oral Epidemiol. 2010; 38:10–18.
Article19. Sabbe D, De Bourdeaudhuij I, Legiest E, Maes L. A cluster-analytical approach towards physical activity and eating habits among 10-year-old children. Health Educ Res. 2008; 23:753–762.
Article20. Kokkevi A, Stefanis C. The epidemiology of licit and illicit substance use among high school students in Greece. Am J Public Health. 1991; 81:48–52.
Article21. Darling H, Reeder AI, McGee R, Williams S. Disposable income, and spending on fast food, alcohol, cigarettes, and gambling by New Zealand secondary school students. J Adolesc. 2006; 29:837–843.22. Griesbach D, Amos A, Currie C. Adolescent smoking and family structure in Europe. Soc Sci Med. 2003; 56:41–52.
Article23. Park MJ, Lee IS, Shin EK, Joung H, Cho SI. The timing of sexual maturation and secular trends of menarchial age in Korean adolescents. Korean J Pediatr. 2006; 49:610–616.
Article24. Kang BS, Kim GS. SPSS 17.0 Statistical analysis for social science. Seoul: Hannarae;2009. p. 608.25. Ministry of Health and Welfare, Korea Centers for Disease Control and Prevention. 2009 Korean Youth Health Risk Behavior Online Survey. Cheongwon: Korea centers for Disease Contrl and Prevention;2009.26. Lalonde MA. A new perspective on the health of Canadian: A working document. Ottawa: Canada Information;1974.27. Kim YH, Kim YS, Kim GB, Kang SG, Park JY. A Causla relation between the negative health behavior and psychological factors in adolescents. Korean J Sport Psychol. 2000; 11:133–150.28. Challier B, Chau N, Prédine R, Choquet M, Legras B. Associations of family environment and individual factors with tobacco, alcohol and illicit drug use in adolescents. Eur J Epidemiol. 2000; 16:33–42.29. Shin BM. Association between stress, oral health behavior and oral health status among 6th grade primary school students in Gangneung city. J Korean Acad Oral Health. 2010; 34:403–410.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Analysis of traumatic dental injury experience and related factors among Korean adolescents: using the 19th (2023) Korea Youth Risk Behavior Survey data
- Effects of health-related behaviors and oral health behaviors on oral disease symptoms in adolescents
- The relationship between pit and fissure sealant (PFS) experience and the socio-economic factors of adolescents before and after coverage by National Health Insurance (NHI)
- The differences of oral health-related behaviors by type of school among high school students in Gangneung city
- The relationship between oral health behaviors and periodontal health status of Korean adolescents
