World J Mens Health.
2014 Aug;32(2):93-98. 10.5534/wjmh.2014.32.2.93.
Magnification-Assisted Subinguinal Varicocelectomy with Testicular Delivery in Children: A Preliminary Report
- Affiliations
-
- 1Department of Anesthesiology and Pain Medicine, Jeju National University Hospital, Jeju National University School of Medicine, Jeju, Korea.
- 2Department of Urology, Inje University Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 3Department of Urology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Urology, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea. scpark@amc.seoul.kr
- KMID: 2320799
- DOI: http://doi.org/10.5534/wjmh.2014.32.2.93
Abstract
- PURPOSE
To evaluate the effectiveness of magnification-assisted subinguinal varicocelectomy (MASV) with testicular delivery in children with severe varicocele.
MATERIALS AND METHODS
We retrospectively analyzed the clinical data of 23 children 15 years or younger (mean age, 12.3+/-1.8 years) who underwent MASV with testicular delivery and ligation of all collateral veins except arteries and deferential veins between January 2010 and January 2014. All patients had grade 3 varicocele on the left side. Varicocelectomy was decided upon due to scrotal hypotrophy (n=14, 60.9%), the existence of mass (n=6, 26.1%, including 1 recurrent case), and discomfort (n=3, 13.0%). The preservation of internal spermatic artery (ISA) was successful in 8 patients (34.8%). The mean follow-up time was 10.8+/-6.6 months.
RESULTS
The surgical success rate of varicocelectomy was 100%. The overall symptom resolution rate was 91.3%. The scrotal mass and discomfort disappeared, but testicular catch-up growth did not occur in 2 among 14 patients with scrotal hypotrophy. The left testis volume increased from 6.5+/-4.3 mL to 10.6+/-7.5 mL (p=0.003). There were no significant inter-group differences in terms of the surgical success rate, symptom resolution, and catch-up growth between the ISA preservation group and the ligation group. None of the subjects demonstrated testicular atrophy or hydrocele after surgery.
CONCLUSIONS
MASV with testicular delivery is an effective and safe method for children with severe varicocele.
Keyword
MeSH Terms
Figure
-
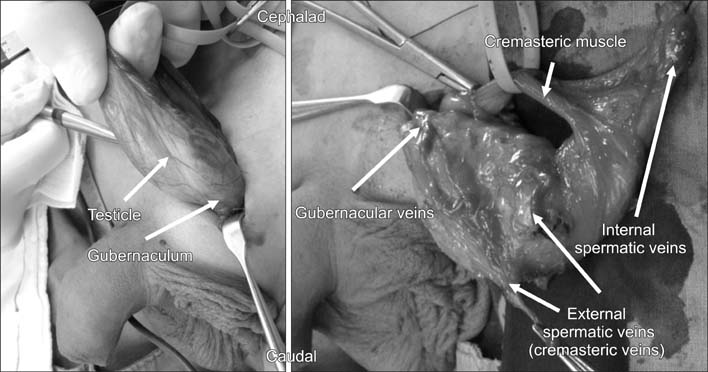
Fig. 1 The process of magnification-assisted subinguinal varicocelectomy with testicular delivery.
Reference
-
1. Camoglio FS, Cervellione RM, Dipaola G, Balducci T, Giacomello L, Zanatta C, et al. Idiopathic varicocele in children. Epidemiological study and surgical approach. Minerva Urol Nefrol. 2001; 53:189–193.2. al-Abbadi K, Smadi SA. Genital abnormalities and groin hernias in elementary-school children in Aqaba: an epidemiological study. East Mediterr Health J. 2000; 6:293–298.3. Hwang Y, Park SW. Epidemiologic study of the prevalence and awareness of cryptorchidism, hydrocele, and varicocele in elementary schools in Gwangju. Korean J Urol. 2009; 50:278–281.
Article4. Belloli G, D'Agostino S, Pesce C, Fantuz E. Varicocele in childhood and adolescence and other testicular anomalies: an epidemiological study. Pediatr Med Chir. 1993; 15:159–162.5. Akbay E, Cayan S, Doruk E, Duce MN, Bozlu M. The prevalence of varicocele and varicocele-related testicular atrophy in Turkish children and adolescents. BJU Int. 2000; 86:490–493.
Article6. Lemack GE, Uzzo RG, Schlegel PN, Goldstein M. Microsurgical repair of the adolescent varicocele. J Urol. 1998; 160:179–181.
Article7. Chehval MJ, Purcell MH. Deterioration of semen parameters over time in men with untreated varicocele: evidence of progressive testicular damage. Fertil Steril. 1992; 57:174–177.
Article8. Lund L, Tang YC, Roebuck D, Lee KH, Liu K, Yeung CK. Testicular catch-up growth after varicocele correction in adolescents. Pediatr Surg Int. 1999; 15:234–237.
Article9. Laven JS, Haans LC, Mali WP, te Velde ER, Wensing CJ, Eimers JM. Effects of varicocele treatment in adolescents: a randomized study. Fertil Steril. 1992; 58:756–762.
Article10. Papanikolaou F, Chow V, Jarvi K, Fong B, Ho M, Zini A. Effect of adult microsurgical varicocelectomy on testicular volume. Urology. 2000; 56:136–139.
Article11. Seo JW, Cho KS, Han SW. Ipsilateral testicular catch-up growth after varicocelectomy in adolescents. Korean J Urol. 2007; 48:731–734.
Article12. Cayan S, Shavakhabov S, Kadioğlu A. Treatment of palpable varicocele in infertile men: a meta-analysis to define the best technique. J Androl. 2009; 30:33–40.
Article13. Al-Said S, Al-Naimi A, Al-Ansari A, Younis N, Shamsodini A, A-sadiq K, et al. Varicocelectomy for male infertility: a comparative study of open, laparoscopic and microsurgical approaches. J Urol. 2008; 180:266–270.
Article14. Beck EM, Schlegel PN, Goldstein M. Intraoperative varicocele anatomy: a macroscopic and microscopic study. J Urol. 1992; 148:1190–1194.
Article15. Murray RR Jr, Mitchell SE, Kadir S, Kaufman SL, Chang R, Kinnison ML, et al. Comparison of recurrent varicocele anatomy following surgery and percutaneous balloon occlusion. J Urol. 1986; 135:286–289.
Article16. Goldstein M, Gilbert BR, Dicker AP, Dwosh J, Gnecco C. Microsurgical inguinal varicocelectomy with delivery of the testis: an artery and lymphatic sparing technique. J Urol. 1992; 148:1808–1811.
Article17. Ramasamy R, Schlegel PN. Microsurgical inguinal varicocelectomy with and without testicular delivery. Urology. 2006; 68:1323–1326.
Article18. Dubin L, Amelar RD. Varicocele size and results of varicocelectomy in selected subfertile men with varicocele. Fertil Steril. 1970; 21:606–609.
Article19. Moon KH, Cho SJ, Kim KS, Park S, Park S. Recurrent varicoceles: causes and treatment using angiography and magnification assisted subinguinal varicocelectomy. Yonsei Med J. 2012; 53:723–728.
Article20. Coolsaet BL. The varicocele syndrome: venography determining the optimal level for surgical management. J Urol. 1980; 124:833–839.
Article21. Abdel-Maguid AF, Othman I. Microsurgical and nonmagnified subinguinal varicocelectomy for infertile men: a comparative study. Fertil Steril. 2010; 94:2600–2603.
Article22. Park K, Cho SY, Kim SW. The surgical difficulty of microsurgical subinguinal varicocelectomy is similar regardless of age. J Urol. 2011; 186:2397–2401.
Article23. Kim KS, Lee C, Song SH, Cho SJ, Park S, Moon KH, et al. Impact of internal spermatic artery preservation during laparoscopic varicocelectomy on recurrence and the catch-up growth rate in adolescents. J Pediatr Urol. 2014; 10:435–440.
Article24. Maghraby HA. Laparoscopic varicocelectomy for painful varicoceles: merits and outcomes. J Endourol. 2002; 16:107–110.
Article25. Choi WS, Kim SW. Current issues in varicocele management: a review. World J Mens Health. 2013; 31:12–20.
Article26. Al-Buheissi SZ, Patel HR, Wazait HD, Miller RA, Nathan S. Predictors of success in surgical ligation of painful varicocele. Urol Int. 2007; 79:33–36.
Article27. Kim JS, Min SK, Jo MK. Effect of varicocele ligation for patients with painful varicocele. Korean J Urol. 2001; 42:732–735.28. Lee HJ, Cheon SH, Ji YH, Moon KH, Kim KS, Park S, et al. Clinical characteristics and surgical outcomes in adolescents and adults with varicocele. Korean J Urol. 2011; 52:489–493.
Article29. Zampieri N, Mantovani A, Ottolenghi A, Camoglio FS. Testicular catch-up growth after varicocelectomy: does surgical technique make a difference. Urology. 2009; 73:289–292.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Recurrent Varicoceles: Causes and Treatment Using Angiography and Magnification Assisted Subinguinal Varicocelectomy
- Testicular Biopsy Histopathology as an Indicator of Successful Restoration of Spermatogenesis after Varicocelectomy in Non-obstructive Azoospermia
- Microsurgical Subinguinal Varicocelectomy
- Comparison of Laparosopic Varicocelectomy with Subinguinal Varicocelectomy
- Microsurgical Subinguinal Varicocelectomy: Comparison of Pediatric and Adult Patients
