Low Grade Pulmonary Lymphomatoid Granulomatosis with an Endobronchial Mass
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea.
- 2Division of Pulmonary Medicine, Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea. gpdush@hanmail.net
- KMID: 2320608
- DOI: http://doi.org/10.4046/trd.2015.78.2.137
Abstract
- Lymphomatoid granulomatosis (LYG) is an angiocentric and angiodestructive neoplastic proliferation of B and T lymphocytes commonly involving the lungs. Epstein-Barr virus is commonly detected in lesional cells. We report a case of a 54-year-old female with underlying monoclonal gammopathy of unknown significance who presented with a 4 week history of dyspnea and cough. Computed tomography scan of the chest showed multiple lung nodules as well as endobronchial narrowing causing atelectasis at the left upper lobe. Bronchoscopic findings revealed obstruction at the lingula segment due to endobronchial mass as a rare presentation. Bronchoscopic biopsy was diagnosed with LYG grade 1. After treatment, the endobronchial mass and lung lesions were completely resolved. However, the patient eventually evolved to malignant lymphoma after 1 year.
Keyword
MeSH Terms
Figure
-
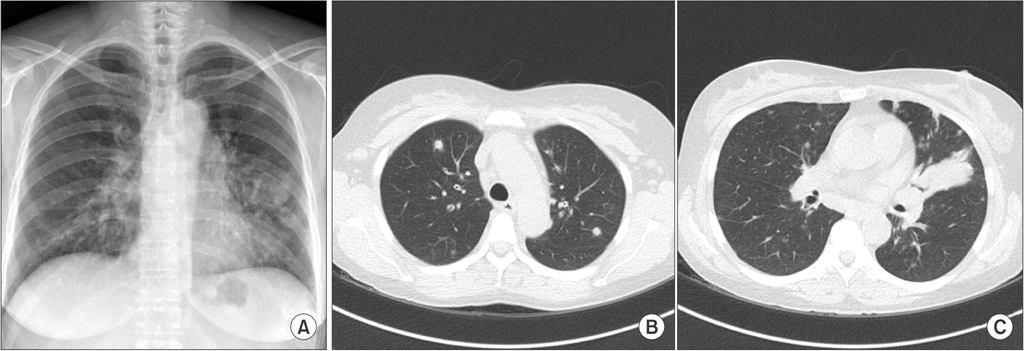
Figure 1 (A) Initial chest posteroanterior image revealing diffuse patchy and nodular densities in the left lower lung. (B, C) Low dose computed tomography scan of chest on admission showing diffused patchy and nodular densities in both lungs and segmental collapse with proximal endobronchial filling defect in left upper lingula segment.
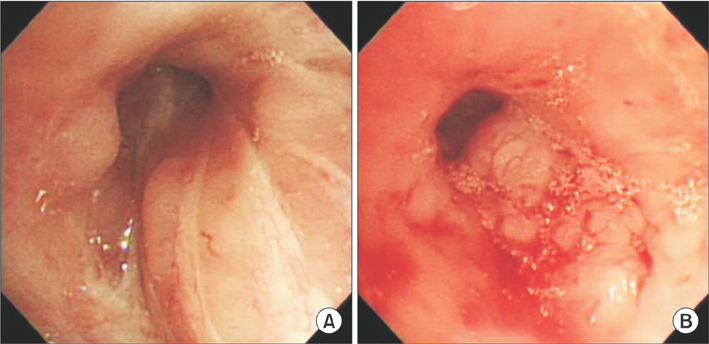
Figure 2 Bronchoscopy showing diffused bronchial nodular lesions with hypervascular mucosal changes and luminal narrowing at right upper lobe (A) and left upper lobe lingular division revealing almost near obstruction (B).
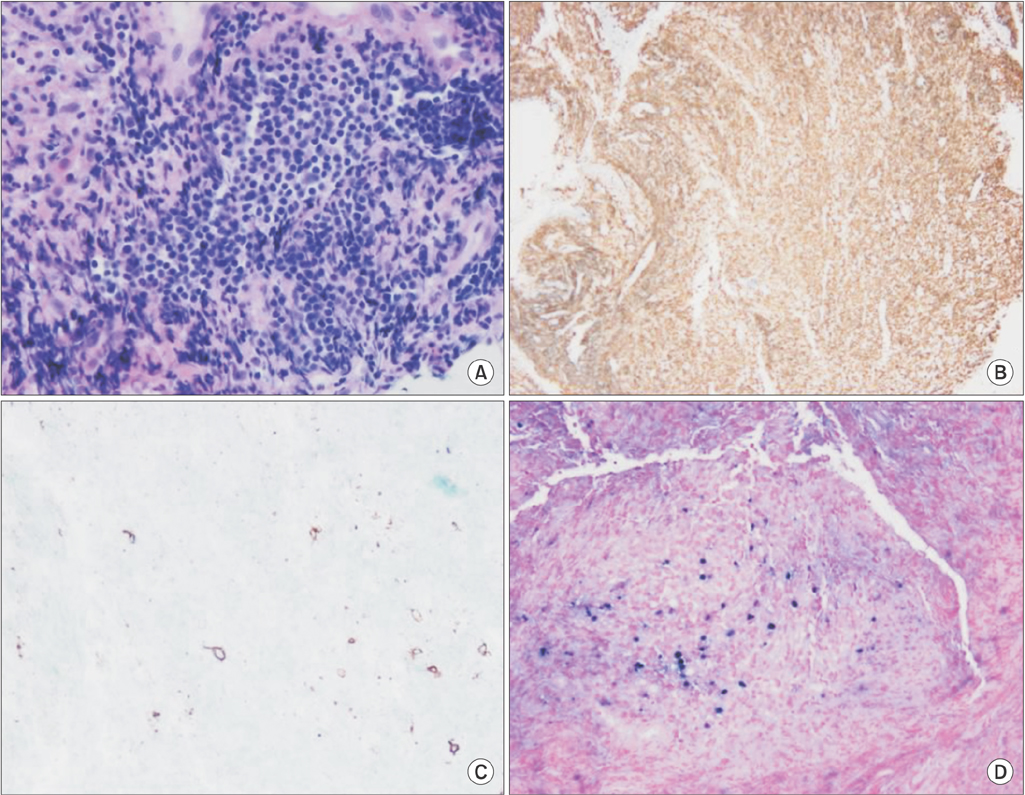
Figure 3 Pathology of endobronchial biopsy showing infiltration of lymphoid cells, scattered plasma cells, and histiocytes (A) at immunohistochemistry, a background of CD4+ T-cells (B) with CD20+ (C), and large atypical B cells with nuclear positivity for Epstein-Barr virus (EBV)-RNA (D) with EBV-encoded RNA probe after in-situ hybridization.
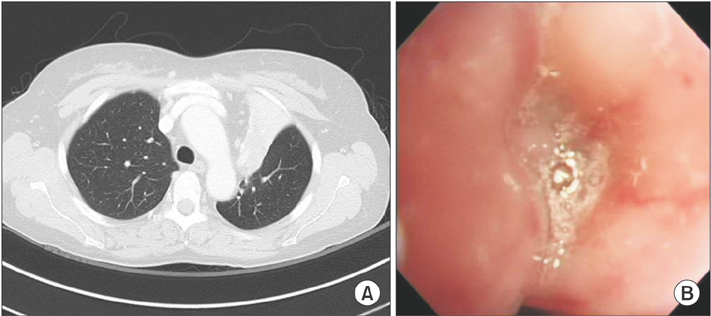
Figure 4 After 8 months of lymphomatoid granulomatosis diagnosis, computed tomography scan of chest showing left upper lobe (LUL) lobar bronchus obstruction and LUL total collapse (A) with bronchoscopy showing total obstruction of LUL bronchus by mass (B).
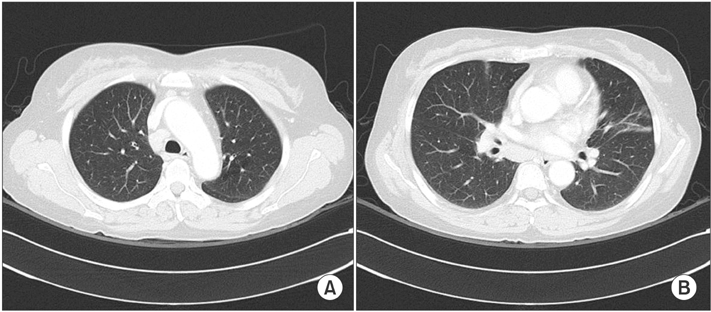
Figure 5 (A, B) Computed tomography scan of chest after cyclophosphamide therapy showing complete regression of endobronchial tumor and atelectasis in left upper lobe as well as multiple lung nodules.
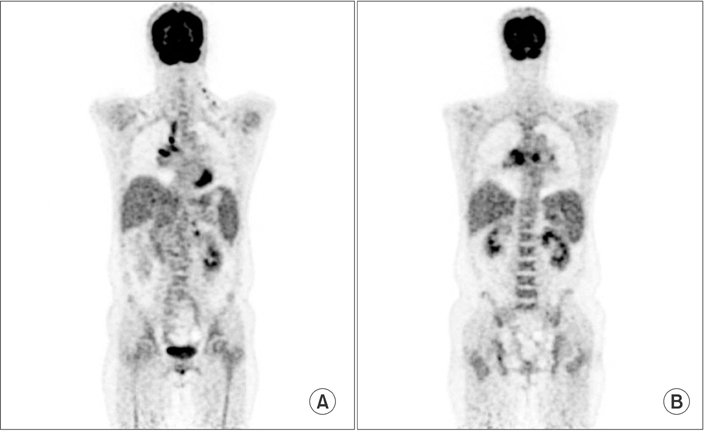
Figure 6 (A, B) Positron emission tomography computed tomography showing fludeoxyglucose uptakes in bilateral lower neck, mediastinum, peribronchial, mesentery and retroperitoneum nodes.
Reference
-
1. Roschewski M, Wilson WH. Lymphomatoid granulomatosis. Cancer J. 2012; 18:469–474.2. Cadranel J, Wislez M, Antoine M. Primary pulmonary lymphoma. Eur Respir J. 2002; 20:750–762.3. Wilson WH, Kingma DW, Raffeld M, Wittes RE, Jaffe ES. Association of lymphomatoid granulomatosis with Epstein-Barr viral infection of B lymphocytes and response to interferonalpha 2b. Blood. 1996; 87:4531–4537.4. Fassas A, Jagannath S, Desikan KR, Shah HR, Shaver R, Waldron J, et al. Lymphomatoid granulomatosis following autologous stem cell transplantation. Bone Marrow Transplant. 1999; 23:79–81.5. Katzenstein AL, Doxtader E, Narendra S. Lymphomatoid granulomatosis: insights gained over 4 decades. Am J Surg Pathol. 2010; 34:e35–e48.6. Hare SS, Souza CA, Bain G, Seely JM, Frcpc , Gomes MM, et al. The radiological spectrum of pulmonary lymphoproliferative disease. Br J Radiol. 2012; 85:848–864.7. Mohyuddin GR, Sultan F, Khaleeq G. A rare presentation of a rare disease: pulmonary lymphomatoid granulomatosis. Case Rep Pulmonol. 2012; 2012:371490.8. Tagliavini E, Rossi G, Valli R, Zanelli M, Cadioli A, Mengoli MC, et al. Lymphomatoid granulomatosis: a practical review for pathologists dealing with this rare pulmonary lymphoproliferative process. Pathologica. 2013; 105:111–116.9. Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. Blood. 2011; 117:5019–5032.10. Jaffe ES, Wilson WH. Lymphomatoid granulomatosis: pathogenesis, pathology and clinical implications. Cancer Surv. 1997; 30:233–248.11. Kwon OJ, Han SK, Shim YS, Kim KY, Han YC, Kim JH, et al. Lymphomatoid granulomatosis: a case report with review of literature. Korean J Intern Med. 1985; 29:124–130.12. Jung HK, Cheon SH, Lee SN, Kim SS. A case of pulomonary lymphomatold granulomatosis. Korean J Med. 1997; 52:247–252.13. Kim EH, Jang HJ, Rhee KH, Han EM, Hugh J, Kim SD, et al. A case of lymphomatoid granulomatosis refractory to various antilymphoma treatment including high dose therapy. Korean J Med. 2007; 72:S332–S337.
