Congenital Cystic Adenomatoid Malformation with Bronchial Atresia in Elderly Patients
- Affiliations
-
- 1Department of Internal Medicine, Hanyang University College of Medicine, Seoul, Korea. hjyoon@hanyang.ac.kr
- 2Department of Internal Medicine, KEPCO, Medical Foundation Hanil General Hospital, Seoul, Korea.
- 3Department of Thoracic and Cardiovascular Surgery, Hanyang University College of Medicine, Seoul, Korea.
Abstract
- Congenital cystic adenomatoid malformation (CCAM) is an uncommon, nonhereditary anomaly caused by arrest of lung. Patients with CCAM may present with respiratory distress as newborns, or may remain asymptomatic until later in life. CCAM type I is rarely found in association with bronchial atresia (BA) in adults; we present such a case. Case: A 54-year-old female presented with chronic cough and blood-tinged sputum. Physical examination and laboratory tests were unremarkable. Chest radiographs and a CT scan of the chest showed multiple large air-filled cysts consistent with a CCAM in the right lower lobe, and an oval-shaped opacity in the distal right middle lobal bronchus. Based on the radiologic findings, right middle lobectomy and a medial basal segmentectomy of the right lower lobe were performed via a thoracotomy. These lesions were consistent with Stocker's Type I CCAM and BA in the different lobes.
MeSH Terms
Figure
-

Figure 1 Simple chest radiography on admission. A patch of opacity is seen in the right lower lung field (arrow).

Figure 2 Computed tomography scan of the chest. (A) Multiple large air-filled cysts consistent with a congenital cystic adenomatoid malformation are evident in the right lower lobe (arrow). (B) An oval-shaped opacity of the distal right middle lobe bronchus can be seen in the low-attenuated right middle lobe with no clear connection between the lesion and the tracheobronchial tree (arrow).

Figure 3 Bronchoscopic examination. The right middle lobe (RML) bronchus is not seen on bronchoscopic examination and there is a suspicious dimpling lesion (arrow) in the proximity of the RML bronchus.
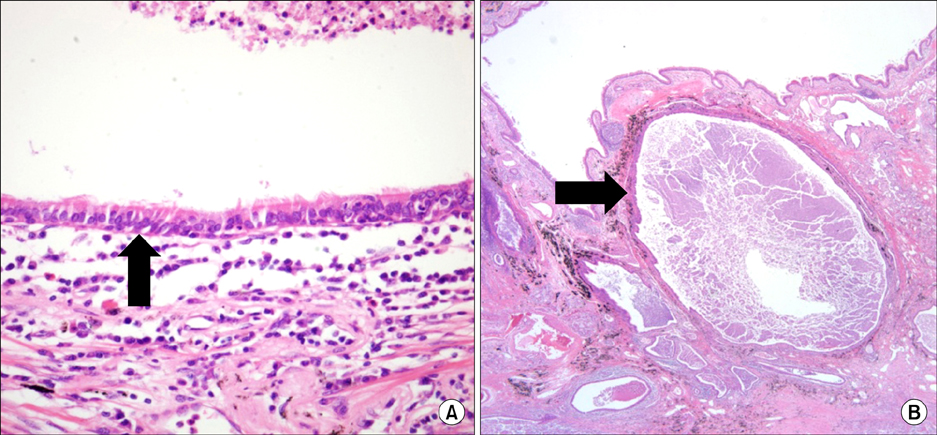
Figure 4 Pathologic examination of the resected lesions. (A) Right lower lobe. Multilocular cystic lesions lined by stratified ciliated columnar epithelium with underlying cartilage and mucus-secreting glands can be seen, together with infiltration of neutrophils, lymphocytes, and plasma cells. These findings are consistent with Stocker's type I congenital cystic adenomatoid malformation and bronchial atresia (H&E stain, ×400). (B) Right middle lobe. The enlarged bronchus and dilated distal alveolar spaces reveal bronchial atresia. A cystically dilated bronchus lined by pseudostratified ciliated columnar epithelium can be seen (H&E stain, ×100).
Reference
-
1. Laberge JM, Flageole H, Pugash D, Khalife S, Blair G, Filiatrault D, et al. Outcome of the prenatally diagnosed congenital cystic adenomatoid lung malformation: a Canadian experience. Fetal Diagn Ther. 2001. 16:178–186.2. Stocker JT, Madewell JE, Drake RM. Congenital cystic adenomatoid malformation of the lung: classification and morphologic spectrum. Hum Pathol. 1977. 8:155–171.3. Liao SL, Lai SH, Hsueh C, Wong KS. Comparing late-onset and neonatally-diagnosed congenital cystic adenomatoid malformation of the lung. Chang Gung Med J. 2010. 33:36–43.4. Discioscio V, Feraco P, Bazzocchi A, Femia R, Romeo C, Fasano L, et al. Congenital cystic adenomatoid malformation of the lung associated with bronchial atresia involving a different lobe in an adult patient: a case report. J Med Case Rep. 2010. 4:164.5. Nagata K, Masumoto K, Tesiba R, Esumi G, Tsukimori K, Norio W, et al. Outcome and treatment in an antenatally diagnosed congenital cystic adenomatoid malformation of the lung. Pediatr Surg Int. 2009. 25:753–757.6. Aslan AT, Yalcin E, Soyer T, Dogru D, Talim B, Ciftci AO, et al. Prenatal period to adolescence: the variable presentations of congenital cystic adenomatoid malformation. Pediatr Int. 2006. 48:626–630.7. Dahabreh J, Zisis C, Vassiliou M, Arnogiannaki N. Congenital cystic adenomatoid malformation in an adult presenting as lung abscess. Eur J Cardiothorac Surg. 2000. 18:720–723.8. Zach MS, Eber E. Adult outcome of congenital lower respiratory tract malformations. Thorax. 2001. 56:65–72.9. Lujan M, Bosque M, Mirapeix RM, Marco MT, Asensio O, Domingo C. Late-onset congenital cystic adenomatoid malformation of the lung: embryology, clinical symptomatology, diagnostic procedures, therapeutic approach and clinical follow-up. Respiration. 2002. 69:148–154.10. West D, Nicholson AG, Colquhoun I, Pollock J. Bronchioloalveolar carcinoma in congenital cystic adenomatoid malformation of lung. Ann Thorac Surg. 2007. 83:687–689.11. d'Agostino S, Bonoldi E, Dante S, Meli S, Cappellari F, Musi L. Embryonal rhabdomyosarcoma of the lung arising in cystic adenomatoid malformation: case report and review of the literature. J Pediatr Surg. 1997. 32:1381–1383.12. Psathakis K, Lachanis S, Kotoulas C, Koutoulidis V, Panagou P, Tsintiris K, et al. The prevalence of congenital bronchial atresia in males. Monaldi Arch Chest Dis. 2004. 61:28–34.13. Riedlinger WF, Vargas SO, Jennings RW, Estroff JA, Barnewolt CE, Lillehei CW, et al. Bronchial atresia is common to extralobar sequestration, intralobar sequestration, congenital cystic adenomatoid malformation, and lobar emphysema. Pediatr Dev Pathol. 2006. 9:361–373.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CONGENITAL CYSTIC ADENOMATOID MALFORMATION TREATED WITH EMERGENCY OPERATION
- Surgical treatment of congenital cystic adenomatoid malformation
- Congenital Cystic Adenomatoid Malformation Associated with Extralobar Pulmonary Sequestration: A case report
- A case of congenital cystic adenomatoid malformation in adult patient
- A case of multicystic dysplastic kidney and cystic adenomatoid malformation of the lung identified as incidental findings
