Pictorial Review of Diffuse Central Airway Diseases: Focus on CT Findings
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Seoul Hospital, Soonchunhyang University College of Medicine, Seoul, Korea. jhhwang@schmc.ac.kr
Abstract
- Various diseases can diffusely involve central airways, including the trachea and main stem bronchi. Central airway abnormalities are frequently not apparent or are overlooked on chest radiographs, even though the patient may have significant symptoms. Recent advances in spiral and multi-detector computed tomography (CT) with multi-planar reconstruction and three-dimensional demonstration, including virtual bronchoscopy, allow for excellent display of central airway anatomy and abnormalities with visualization of accurate locations of lesions. Early detection and proper diagnosis of airway diseases based on various radiographic findings will help determine appropriate treatment, including surgical planning and evaluation of treatment response. Herein we describe and illustrate the imaging findings of a wide spectra of diffuse central airway diseases.
MeSH Terms
Figure
-
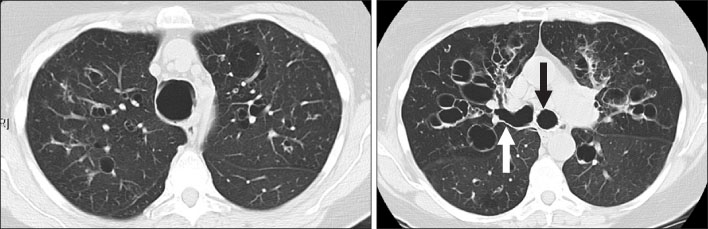
Figure 1 Tracheobronchomegaly in a 47-year-old man. CT scan (5-mm collimation) shows marked dilatation of trachea and both main bronchi with "corrugated" appearance (arrows). Trachea measured 3.9×3.6 cm in diameter.

Figure 2 Kartagener syndrome in a 52-year-old woman. (A) CT shows mucosal thickening and opacification of paranasal sinuses consistent with sinusitis. (B) Posteroanterior chest radiograph shows dextrocardia, situs inversus, diffuse bronchial wall thickening with bronchiectasis. (C) HRCT reveals bilateral bronchiectasis with bronchial wall thickening and centrilobular micronodules representing mucoid impaction.

Figure 3 Allergic bronchopulmonary aspergillosis (ABPA) in a 42-year-old woman. HRCT scan demonstrates finger-in-glove increased opacity (arrows) in right upper lobe resulting from mucoid impaction in bronchi.

Figure 4 Tracheomalacia in a 63-year-old man. Expiratory CT scan demonstrates excessive (>50%) reduction in tracheal cross-sectional area ("frown sign") (arrow).
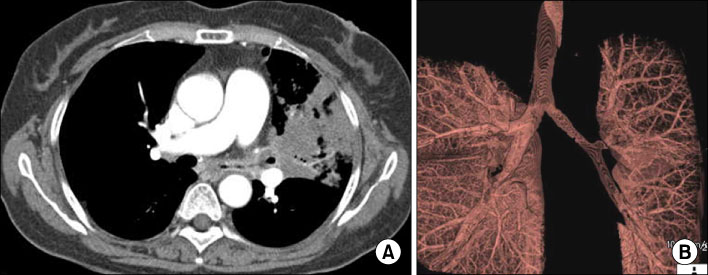
Figure 5 Endobronchial tuberculosis in a 35-year-old woman. (A) Axial CT scan shows diffuse irregular luminal narrowing with enhancing wall thickening in left upper lobar bronchus. (B) CT scan (3-mm collimation) with volume rendering (VR) image demonstrates diffuse irregular luminal narrowing in left central airways.

Figure 6 Tracheobronchopathia osteochondroplastica in a 45-year-man. Nonenhanced axial CT scan demonstrates nodularity of the tracheal wall resulting from thickening and calcification of tracheal cartilage that spares posterior wall (arrow).
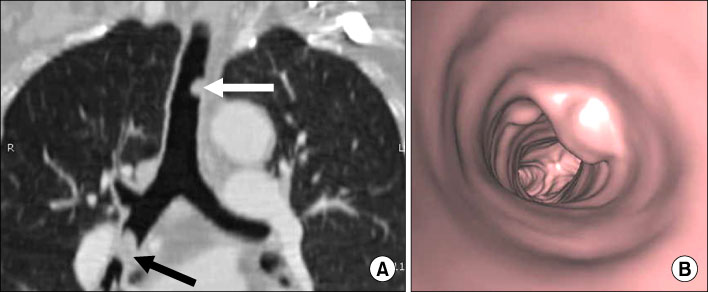
Figure 7 Tracheobronchial papillomatosis in a 49-year-old man. (A) CT scan (3-mm collimation) with coronal multi-planar reconstruction (MPR) image shows multiple polypoid tracheobronchial nodules (arrows). (B) Virtual bronchoscopy demonstrates multiple lobulated intraluminal nodules in trachea and bronchi.

Figure 8 Squamous cell carcinoma of the trachea in a 65-year-old woman. Nonenhanced CT (3-mm collimation) axial CT scan shows irregular intraluminal protruding mass arising from left posterior wall of the lower trachea (arrow), which causes marked tracheal luminal narrowing.

Figure 9 Adenoid cystic carcinoma of left upper lobe bronchus. Axial CT scan at the level of pulmonary trunk reveals circumferential thickening and mass in left upper lobar bronchus producing diffuse luminal narrowing (arrows).

Figure 10 Anthracofibrosis in a 76 year-old woman. Axial CT scan (3-mm collimation) shows multifocal peribronchial cuffs of soft tissue with irregular or smooth luminal narrowing (arrows). A calcified subcarinal lymph node is also seen.
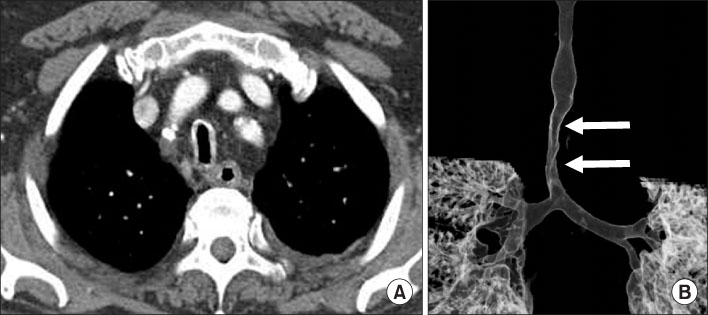
Figure 11 Saber sheath trachea. (A) Axial CT scan (3-mm collimation) at thoracic inlet reveals that sagittal-to-coronal diameter ratio of intrathoracic trachea exceeds 2:1. (B) Coronal shaded-surface-display image shows side to side narrowing of the trachea at level of thoracic inlet (arrows). Note that extrathoracic trachea is normal in diameter.

Figure 12 Relapsing polychondritis in a 42-year-old man. Nonenhanced axial CT scan (5-mm collimation) shows thickening of cartilaginous portion of trachea and bronchi, which is associated with diffuse luminal narrowing. Characteristically sparing of posterior membranous wall is also seen.
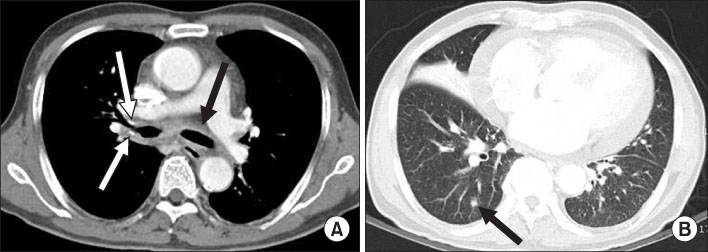
Figure 13 Amyloidosis in a 70 year-old man. (A) CT scan (5-mm collimation) at level of left main bronchus reveals diffuse circumferential bronchial wall thickening. High attenuation areas in bronchial wall likely represent calcification (arrows). (B) Lung window image shows segmental atelectasis in right middle lobe, a nodule in right lower lobe suggestive of an amyloidoma (arrow). Pericardial effusion is also seen.

Figure 14 Tuberculous lymphadenitis in a 33-year-old man. (A, B) Contrast enhanced axial scan reveal conglomerated lymphadenopathy at right paratracheal, subcarinal and hilar areas, which show low density central necrosis with peripheral rim enhancement. (C) Coronal reformation image shows diffuse smooth luminal narrowing of tracheobronchi caused by mediastinal and right hilar lymphadenopathy.
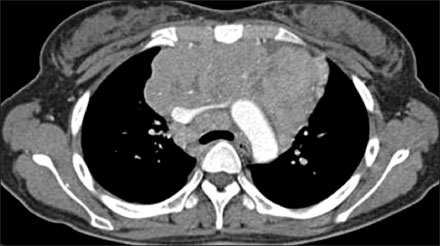
Figure 15 Hodgkin's lymphoma in a 29-year-old woman. Axial CT scan (3-mm collimation) demonstrates multiple round or bulky matted soft tissue masses in anterior mediastinum and paratracheal area with diffuse encasement of mediastinal greater vessels and central airways. Diffuse smooth luminal narrowing of tracheobronchial trees is seen.
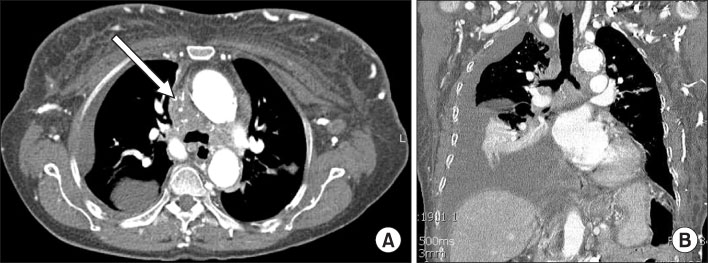
Figure 16 Fibrosing mediastinitis in a 69-year-old woman. (A, B) Contrast enhanced (3-mm collimation) axial and coronal CT scans show soft tissue mass at both paratracheal and subcarinal areas, which is associated with occlusion of superior vena cava (arrow in A) with collateral vessels and soft tissue edema in chest wall. Note irregular luminal narrowing at lower trachea and both main bronchi due to extrinsic compression.
Reference
-
1. Kwong JS, Müller NL, Miller RR. Diseases of the trachea and main-stem bronchi: correlation of CT with pathologic findings. Radiographics. 1992. 12:645–657.2. Marom EM, Goodman PC, McAdams HP. Diffuse abnormalities of the trachea and main bronchi. AJR Am J Roentgenol. 2001. 176:713–717.3. Hansell DM, Armstrong P, Lynch DA, McAdams HP, editors. Chapter 12. Airway disease. Imaging of diseases of the chest. 2005. 4th ed. Philadelphia: Elsevier Mosby;711–783.4. Rossi SE, Franquet T, Volpacchio M, Giménez A, Aguilar G. Tree-in-bud pattern at thin-section CT of the lungs: radiologic-pathologic overview. Radiographics. 2005. 25:789–801.5. Boiselle PM, Ernst A. Tracheal morphology in patients with tracheomalacia: prevalence of inspiratory lunate and expiratory "frown" shapes. J Thorac Imaging. 2006. 21:190–196.6. Prince JS, Duhamel DR, Levin DL, Harrell JH, Friedman PJ. Nonneoplastic lesions of the tracheobronchial wall: radiologic findings with bronchoscopic correlation. Radiographics. 2002. 22:S215–S230.7. Marom EM, Goodman PC, McAdams HP. Focal abnormalities of the trachea and main bronchi. AJR Am J Roentgenol. 2001. 176:707–711.8. Spizarny DL, Shepard JA, McLoud TC, Grillo HC, Dedrick CG. CT of adenoid cystic carcinoma of the trachea. AJR Am J Roentgenol. 1986. 146:1129–1132.9. Park HJ, Park SH, Im SA, Kim YK, Lee KY. CT differentiation of anthracofibrosis from endobronchial tuberculosis. AJR Am J Roentgenol. 2008. 191:247–251.10. Rossi SE, McAdams HP, Rosado-de-Christenson ML, Franks TJ, Galvin JR. Fibrosing mediastinitis. Radiographics. 2001. 21:737–757.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- CT Findings of Central Airway Lesions Causing Airway Stenosis-Visualization and Quantification: A Pictorial Essay
- Neurological Complications Following Liver Transplant: A Pictorial Review of Radiological and Clinical Findings
- Multi-Detector Row CT of the Central Airway Disease
- Imaging Findings of Coronary Artery Fistula in Children: A Pictorial Review
- Non-Neoplastic Disorders of the Esophagus
