Tuberc Respir Dis.
2010 Jul;69(1):52-55.
A Case of Atypical Distribution of Pulmonary Tuberculosis in Bedridden Patient with Quadriplegia
- Affiliations
-
- 1Respiratory Division, Department of Internal Medicine, Gumi, Korea. hwangpark@hanmail.net
- 2Department of Radiology, Soonchunhyang University Gumi Hospital, Soonchunhyang University School of Medicine, Gumi, Korea.
Abstract
- Pulmonary tuberculosis has intermediate prevalence in Korea. It is known that tuberculosis infection predominantly involves the upper lobes, based on the fact that multiplication of Mycobacterium tuberculosis is favored in areas with decreased pulmonary blood flow, impaired lymphatic drainage, and high oxygen tension. We report this case of a 40-year-old man who was brought to our hospital with hemoptysis and dyspnea. Prior to admission, the patient had been in a bedridden state for 15 years due to an injury of the cervical spine 4~5. A 3-Dimensional computed tomography showed predominantly longitudinal distribution of centrilobular nodules along the anterior chest wall, in the left lung. MTB-PCR and AFB culture of bronchial washing fluid revealed pulmonary tuberculosis. This case shows that long-standing supine posture and decreased motion of the anterior chest wall may change the distribution of preferential infection site of Mycobacterium tuberculosis in the lung, resulting in a ventral predominance of tuberculosis infection in the quadriplegic patient.
MeSH Terms
Figure
-
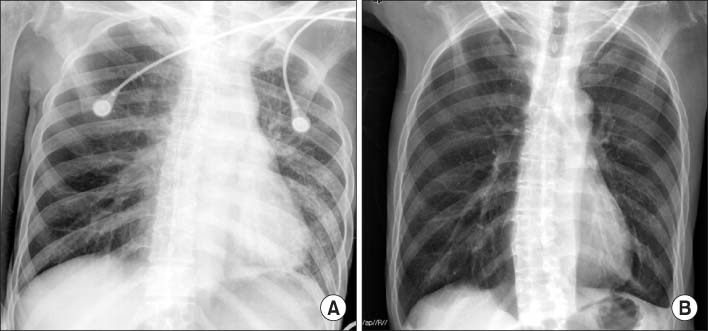
Figure 1 Chest X-ray shows (A) peribronchial patchy infiltration in left upper and lower lung fields on admission, and (B) much cleared lung field after antituberculosis treatment for 9 months.
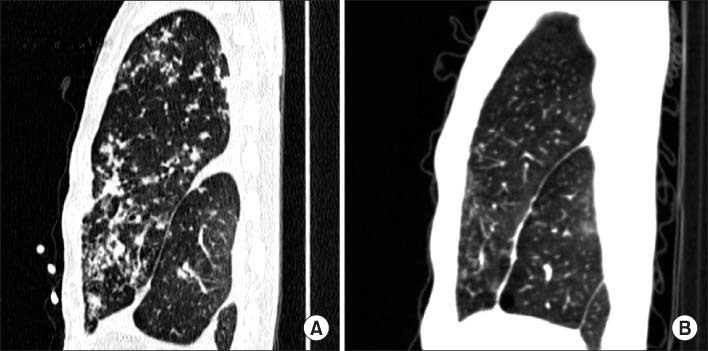
Figure 2 Sagittal section of lung setting shows (A) patchy and centrilobular infiltration prominently in anterior chest wall of left lung field, and (B) much cleared lung field after antituberculosis treatment for 9 months.
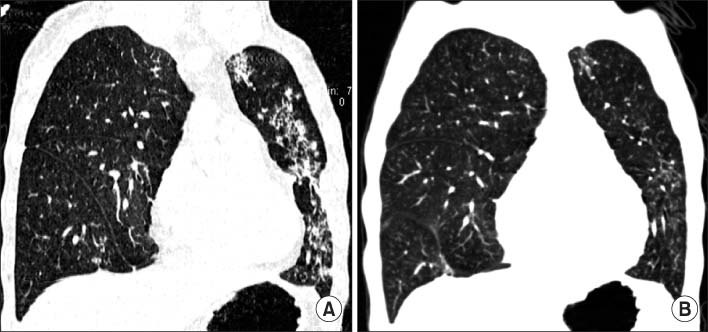
Figure 3 Coronal section of lung setting shows (A) patchy and centrilobular infiltration in line along anterior chest wall of left lung field, and (B) much cleared lung field after antituberculosis treatment for 9 months.
Reference
-
1. TB prevalence and incidence: Republic of Korea [Internet]. World Health Organization. c2010. cited 2010 April 1. Geneva: World Health Organization;Available from: http://www.who.int/countries/kor/en.2. Meylan PR, Richman DD, Kornbluth RS. Reduced intracellular growth of mycobacteria in human macrophages cultivated at physiologic oxygen pressure. Am Rev Respir Dis. 1992. 145:947–953.3. Perez-Guzman C, Torres-Cruz A, Villarreal-Velarde H, Vargas MH. Progressive age-related changes in pulmonary tuberculosis images and the effect of diabetes. Am J Respir Crit Care Med. 2000. 162:1738–1740.4. Cegielski JP, Chin DP, Espinal MA, Frieden TR, Rodriquez Cruz R, Talbot EA, et al. The global tuberculosis situation. Progress and problems in the 20th century, prospects for the 21st century. Infect Dis Clin North Am. 2002. 16:1–58.5. Jeong YJ, Lee KS. Pulmonary tuberculosis: up-to-date imaging and management. AJR Am J Roentgenol. 2008. 191:834–844.6. Lee KS, Im JG. CT in adults with tuberculosis of the chest: characteristic findings and role in management. AJR Am J Roentgenol. 1995. 164:1361–1367.7. Chan CH, Woo J, Or KK, Chan RC, Cheung W. The effect of age on the presentation of patients with tuberculosis. Tuber Lung Dis. 1995. 76:290–294.8. Umeki S. Comparison of younger and elderly patients with pulmonary tuberculosis. Respiration. 1989. 55:75–83.9. Houben EN, Nguyen L, Pieters J. Interaction of pathogenic mycobacteria with the host immune system. Curr Opin Microbiol. 2006. 9:76–85.10. MacGregor RR. Tuberculosis: from history to current management. Semin Roentgenol. 1993. 28:101–108.11. West JB, Dollery CT. Distribution of blood flow and ventilation-perfusion ratio in the lung, measured with radioactive carbon dioxide. J Appl Physiol. 1960. 15:405–410.12. Anthonisen NR, Milic-Emili J. Distribution of pulmonary perfusion in erect man. J Appl Physiol. 1966. 21:760–766.13. Goodwin RA, Des Prez RM. Apical localization of pulmonary tuberculosis, chronic pulmonary histoplasmosis, and progressive massive fibrosis of the lung. Chest. 1983. 83:801–805.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Atypical Form of Multiple Spinal Tuberculosis
- Atypical Presentation of Spinal Tuberculosis Misadiagnosed as Metastatic Spine Tumor
- A Case of Tuberculosis Verrucosa Cutis with Ulcer in a Patient with Pulmonary Tuberculosis
- Radiographic Findings of Pulmonary Tuberculosis in Non-AIDS Immunocompromised adult Patients: Comparison with Immunocompetent Adult Patients
- Tuberculosis Verrucosa Cutis in a Patient with Pulmonary Tuberculosis
