Tuberc Respir Dis.
2010 Jan;68(1):1-5.
18F-FDG Positron Emission Tomography in Patients with Concomitant Malignancy and Tuberculoma
- Affiliations
-
- 1Division of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shimts@amc.seoul.kr
- 2Department of Nuclear Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Abstract
- BACKGROUND
To analyze the result of 18F-FDG positron emission tomography (PET) in patients with a concomitant malignancy and tuberculoma in a tuberculosis (TB)-endemic area.
METHODS
Twelve patients with a concomitant malignancy and tuberculoma, who underwent whole-body 18F-FDG PET, were evaluated retrospectively. The maximal standardized uptake values (SUVmax) of the malignancy and tuberculoma were compared. In 6 patients, 18F-FDG PET was repeated during the anti-TB treatment and the changes in SUVmax were analyzed.
RESULTS
Of the 12 patients, 10 were male. The mean age was 67.2+/-7.9 years. Tuberculomas were located in the lung (n=10) and lymph nodes (n=2), and tumors were located in the lung (n=6), colon (n=3), stomach (n=1), ovary (n=1) and liver (n=1). Although the mean SUVmax of malignant lesions was higher than that of tuberculomas (5.2+/-3.2 vs 3.5+/-2.0), the difference was not significant. In 4 patients, the SUVmax was higher in the tuberculoma than the tumor. After anti-TB treatment in 6 patients, the mean SUVmax of the tuberculomas decreased significantly, from 3.5+/-2.0 to 1.6+/-0.9 (p=0.028).
CONCLUSION
In patients with a concomitant malignancy and tuberculoma, SUVmax alone could not differentiate between them. However, 18F-FDG PET may be useful in monitoring the response to anti-TB treatment.
Keyword
MeSH Terms
Figure
-
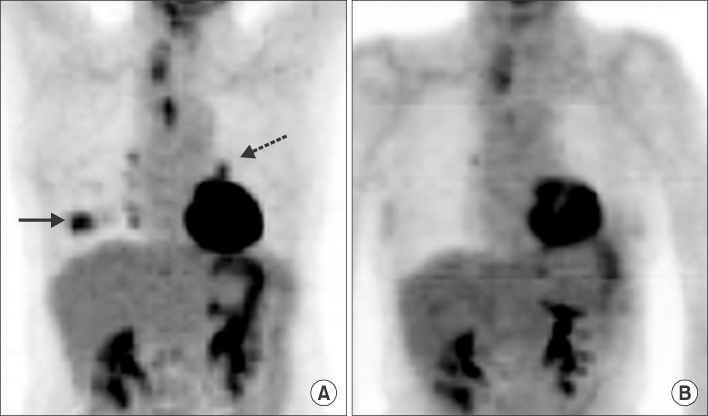
Figure 1 Serial PET scan results in a representative patient with concomitant lung cancer and tuberculoma. A (Baseline) and B (After treatment). Lung cancer (solid arrow) and tuberculoma (dotted arow) disappeared after treatment. The lung cancer was removed by lobectomy and the tuberculoma was treated with first-line anti-tuberculosis drugs.
Reference
-
1. Reske SN, Kotzerke J. FDG-PET for clinical use: results of the 3rd German Interdisciplinary Consensus Conference, "Onko-PET III", 21 July and 19 September 2000. Eur J Nucl Med. 2001. 28:1707–1723.2. Chang JM, Lee HJ, Goo JM, Lee HY, Lee JJ, Chung JK, et al. False positive and false negative FDG-PET scans in various thoracic diseases. Korean J Radiol. 2006. 7:57–69.3. Sochocky S. Tuberculoma of the lung. Am Rev Tuberc. 1958. 78:403–410.4. Goo JM, Im JG, Do KH, Yeo JS, Seo JB, Kim HY, et al. Pulmonary tuberculoma evaluated by means of FDG PET: findings in 10 cases. Radiology. 2000. 216:117–121.5. Hofmeyr A, Lau WF, Slavin MA. Mycobacterium tuberculosis infection in patients with cancer, the role of 18-fluorodeoxyglucose positron emission tomography for diagnosis and monitoring treatment response. Tuberculosis (Edinb). 2007. 87:459–463.6. Yen RF, Chen KC, Lee JM, Chang YC, Wang J, Cheng MF, et al. 18F-FDG PET for the lymph node staging of non-small cell lung cancer in a tuberculosis-endemic country: is dual time point imaging worth the effort? Eur J Nucl Med Mol Imaging. 2008. 35:1305–1315.7. An YS, Sun JS, Park KJ, Hwang SC, Park KJ, Sheen SS, et al. Diagnostic performance of 18F-FDG PET/CT for lymph node staging in patients with operable non-small-cell lung cancer and inflammatory lung disease. Lung. 2008. 186:327–336.8. Low SY, Eng P, Keng GH, Ng DC. Positron emission tomography with CT in the evaluation of non-small cell lung cancer in populations with a high prevalence of tuberculosis. Respirology. 2006. 1:84–89.9. Hara T, Kosaka N, Suzuki T, Kudo K, Niino H. Uptake rates of 18F-fluorodeoxyglucose and 11C-choline in lung cancer and pulmonary tuberculosis: a positron emission tomography study. Chest. 2003. 124:893–901.10. Park IN, Ryu JS, Shim TS. Evaluation of therapeutic response of tuberculoma using F-18 FDG positron emission tomography. Clin Nucl Med. 2008. 33:1–3.11. Demura Y, Tsuchida T, Uesaka D, Umeda Y, Morikawa M, Ameshima S, et al. Usefulness of 18F-fluorodeoxyglucose positron emission tomography for diagnosing disease activity and monitoring therapeutic response in patients with pulmonary mycobacteriosis. Eur J Nucl Med Mol Imaging. 2009. 36:632–639.12. Davis SL, Nuermberger EL, Um PK, Vidal C, Jedynak B, Pomper MG, et al. Noninvasive pulmonary [18F]-2-fluoro-deoxy-D-glucose positron emission tomography correlates with bactericidal activity of tuberculosis drug treatment. Antimicrob Agents Chemother. 2009. 53:4879–4884.13. Lee HS, Oh JY, Lee JH, Yoo CG, Lee CT, Kim YW, et al. Response of pulmonary tuberculomas to anti-tuberculous treatment. Eur Respir J. 2004. 23:452–455.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- 18F-FDG PET/CT Findings in a Breast Cancer Patient with Concomitant Tuberculous Axillary Lymphadenitis
- Supraclavicular Lymph Node Metastasis from Various Malignancies: Assessment with 18F-Fluorodeoxyglucose Positron Emission Tomography/CT, Contrast-Enhanced CT and Ultrasound
- Perirenal 18F-FDG Uptake in a Patient with a Pheochromocytoma
- Random Synchronous Malignancy in Male Breast: A Case Report
- Lymphocytic Thyroiditis Presenting as a Focal Uptake on 18F-Fluorodeoxyglucose Positron Emission Tomography: A Case Report
