Synchronous Roentgenographically Occult Lung Carcinoma Treated with Argon Plasma Coagulation in a Patient with Resectable Primary Lung Cancer
- Affiliations
-
- 1Department of Internal Medicine, Konyang University College of Medicine, Daejon, Korea. sk1609@hanmail.net
- 2Department of Chest Surgery, Konyang University College of Medicine, Daejon, Korea.
- 3Department of Pathology, Konyang University College of Medicine, Daejon, Korea.
- 4Department of Diagnostic Radiology, Konyang University College of Medicine, Daejon, Korea.
Abstract
- We treated synchronous double primary lung cancers, where one site resulted from CIS disease, with lobectomy and argon plasma coagulation (APC) in a patient who couldn't tolerate pneumonectomy, which resulted in a reduction of the extent of surgery. APC could be a reasonable alternative for CIS disease of lung in inoperable patients.
Keyword
Figure
-
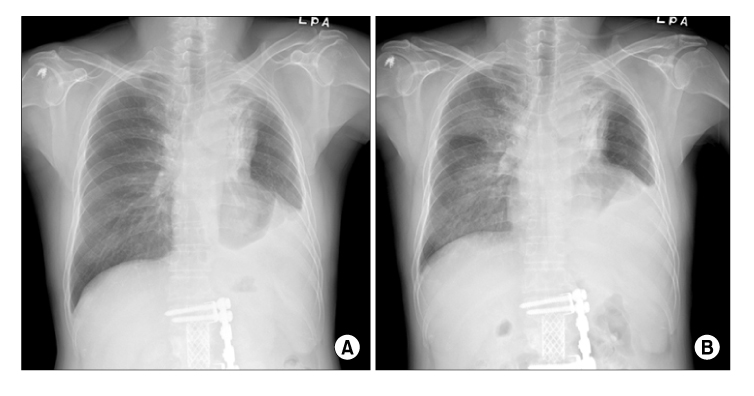
Figure 1 Preoperative images of CT showed (A) about 3.7×2.7 cm sized heterogenous enhancing low density mass with total obstruction of anterior segmental bronchus of right upper lung (solid arrow), (B) proximal portion of right middle and lower bronchus is unremarkable (dashed arrow).
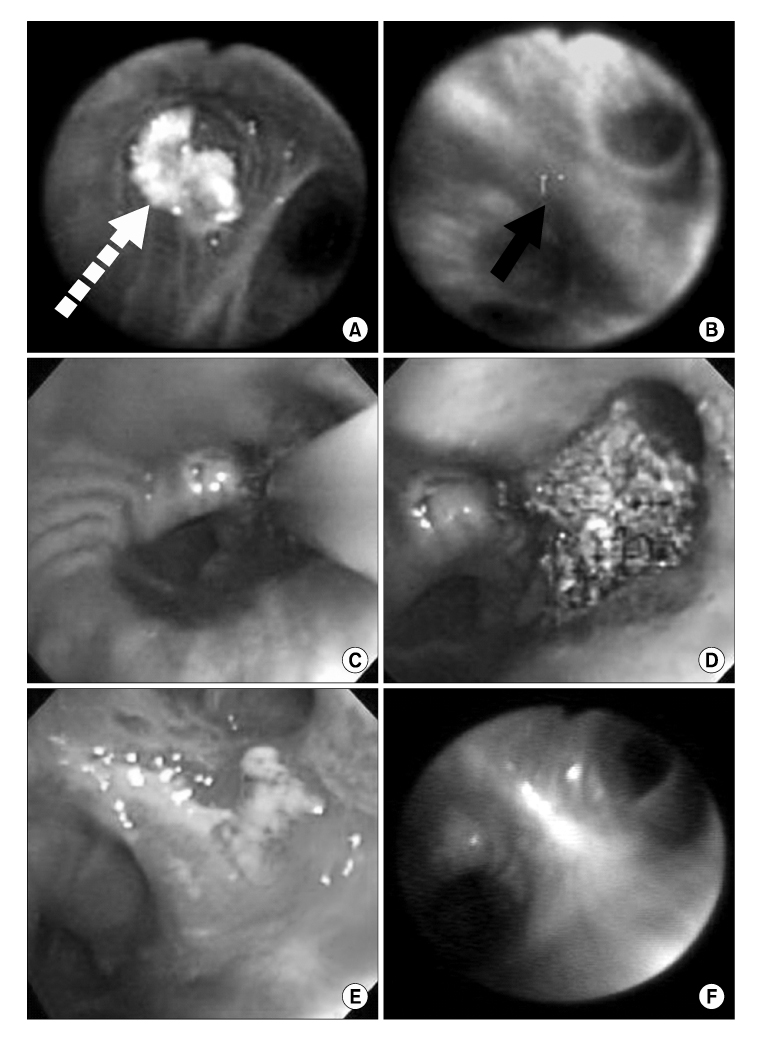
Figure 2 Initial bronchoscopy showed (A) intraluminal mass in RB3 (white dashed arrow) by conventional bronchoscopy, and (B) 'loss of autofluorescence' in superior segment of right lower bronchus (black solid arrow) by autofluorescence bronchoscopy. (C) APC was performed on the superior segment of right lower bronchus, (D) bronchoscopy immediate after APC showed debris, (E) and after two and half weeks ulcerative and mild edematous changes were shown. (F) No evidence of recurrence was shown on bronchoscopy on 3 months post-APC.
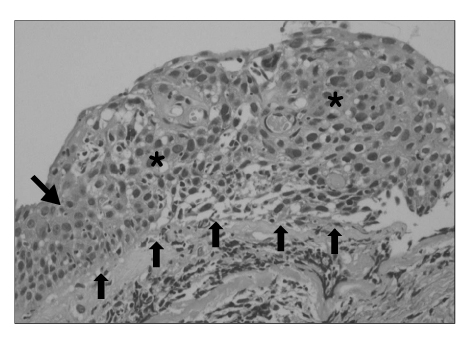
Figure 3 The report from pathologist revealed 'carcinoma in situ' for superior segment of right lower bronchus. The five small upward arrows shows intact basement membrane, and the region marked as '*' is filled with cancer cells with mitosis, pleomorphism. The downward arrow (left middle) revealed normal stratified squamous epithelium (H&E stain, ×200).
Reference
-
1. Lam S, MacAulay C, Hung J, LeRiche J, Profio AE, Palcic B. Detection of dysplasia and carcinoma in situ with a lung imaging fluorescence endoscope device. J Thorac Cardiovasc Surg. 1993. 105:1035–1040.2. Pierard P, Vermylen P, Bosschaerts T, Roufosse C, Berghmans T, Sculier JP, et al. Synchronous roentgenographically occult lung carcinoma in patients with resectable primary lung cancer. Chest. 2000. 117:779–785.3. Venmans BJ, van Boxem TJ, Smit EF, Postmus PE, Sutedja TG. Outcome of bronchial carcinoma in situ. Chest. 2000. 117:1572–1576.4. Johanns W, Luis W, Janssen J, Kahl S, Greiner L. Argon plasma coagulation (APC) in gastroenterology: experimental and clinical experiences. Eur J Gastroenterol Hepatol. 1997. 9:581–587.5. Freitag L. Interventional endoscopic treatment. Lung Cancer. 2004. 45:S235–S238.6. Morice RC, Ece T, Ece F, Keus L. Endobronchial argon plasma coagulation for treatment of hemoptysis and neoplastic airway obstruction. Chest. 2001. 119:781–787.7. Okada S, Yamauchi H, Ishimori S, Satoh S, Sugawara H, Tanaba Y. Endoscopic surgery with a flexible bronchoscope and argon plasma coagulation for tracheobronchial tumors. J Thorac Cardiovasc Surg. 2001. 121:180–182.8. Stephens KE Jr, Wood DE. Bronchoscopic management of central airway obstruction. J Thorac Cardiovasc Surg. 2000. 119:289–296.9. Hooper RG. Electrocautery in endobronchial therapy. Chest. 2000. 117:1820–1821.10. Ledingham SJ, Goldstraw P. Diathermy resection and radioactive gold grains for palliation of obstruction due to recurrence of bronchial carcinoma after external irradiation. Thorax. 1989. 44:48–51.11. Sutedja G, Schramel F, Postmus PE. Bronchoscopic treatment modalities in lung cancer, indications and limitations. Ann Oncol. 1995. 6:951–952.12. Shah H, Garbe L, Nussbaum E, Dumon JF, Chiodera PL, Cavaliere S. Benign tumors of the tracheobronchial tree. Endoscopic characteristics and role of laser resection. Chest. 1995. 107:1744–1751.13. Schuurman B, Postmus PE, van Mourik JC, Risse EK, Sutedja TG. Combined use of autofluorescence bronchoscopy and argon plasma coagulation enables less extensive resection of radiographically occult lung cancer. Respiration. 2004. 71:410–411.14. Kato H, Konaka C, Ono J, Kawate N, Nishimiya K, Shinohara H, et al. Preoperative laser photodynamic therapy in combination with operation in lung cancer. J Thorac Cardiovasc Surg. 1985. 90:420–429.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Synchronous Primary Lung Cancer with Differrent Squamous cell Carcinoma: One Case Report
- Tripe synchronous primary lung cancer: one case report
- Surgical Treatment for Multiple Primary Lung Cancer: Report of 2 cases
- Multiple primary lung cancer: Synchronous small cell lung carcinoma and squamous cell carcinoma
- Synchronous double cancer of rectal non-Hodgkin lymphoma and lung cancer: 1 case report
