A Case of Radiolucent Foreign Body (Temporary Resin Bridge) Aspiration Accompanied by Inflammatory Polyps
- Affiliations
-
- 1Department of Internal Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. mdlee@catholic.ac.kr
Abstract
- This case demonstrates the rare occurrence of a radiolucent temporary resin bridge aspiration in adults while they are in a conscious and awaken state and the resultant formation of inflammatory polyps. Although no unique findings were noted in a chest x-ray, careful history taking accompanied by physical examinations can lead to clinical suspicion of foreign body aspiration in an earlier stage. Moreover, flexible bronchoscopy is a tool useful not only for the evaluation process but also for managing the aspirated foreign material.
Keyword
MeSH Terms
Figure
-
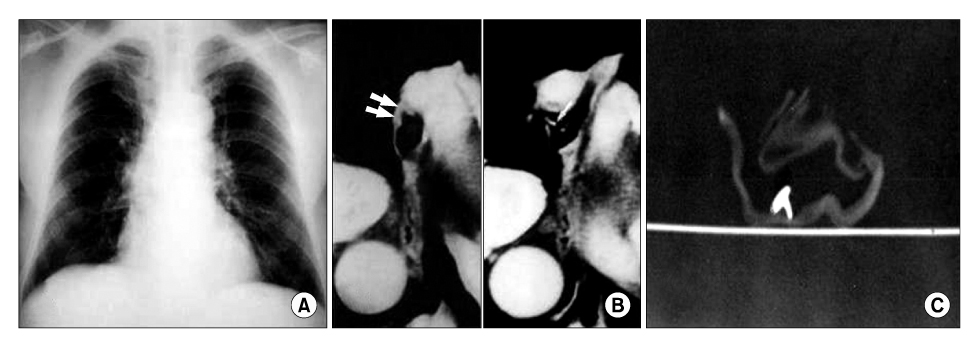
Figure 1 Initial chest X-ray shows no definite abnormalities (A). Chest CT shows focal wall thickening and linear high density in the lumen of right bronchus intermedius (B). After removal of the foreign body, CT was performed with the bronchial foreign body wrapped with gauze. In this CT, the foreign body is of high density (C).
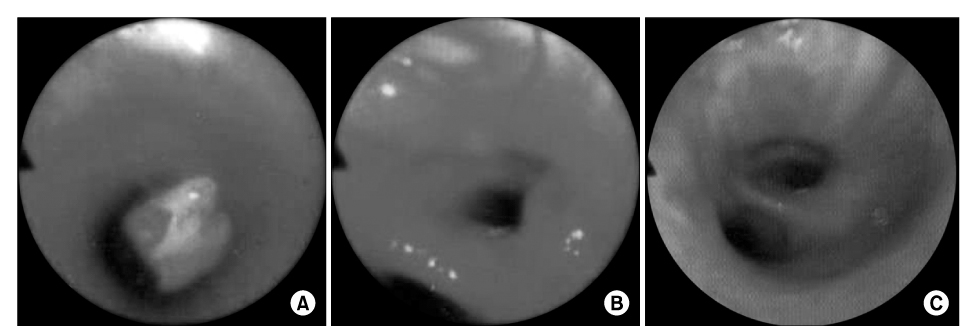
Figure 2 Flexible fiberoptic bronchoscopy, demonstrating a white-yellowish foreign material in the right bronchus intermedius (A). After removal of a foreign material, multiple polypoid endobronchial masses were observed distal to the impacted site (B). Follow up bronchoscopy performed two months later shows mild mucosal elevations with hyperemic changes (C).
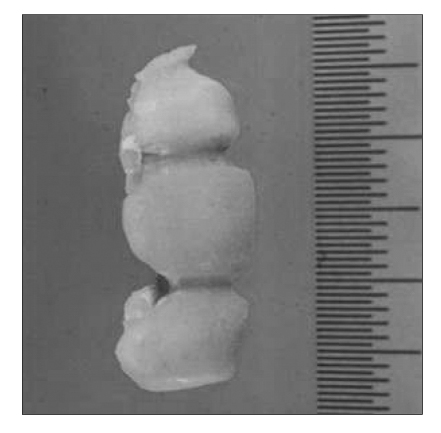
Figure 3 Foreign body removed by flexible fiberoptic bronchoscopy, was revealed to be a temporary resin bridge.
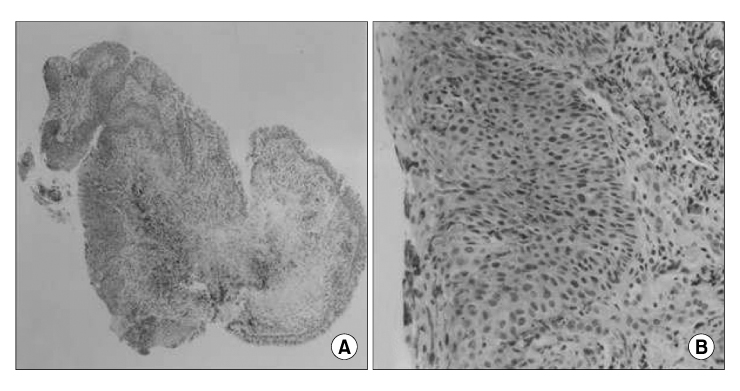
Figure 4 Biopsy specimen of polypoid mass shows scquamous metaplasia with focal dysplastic changes, granulation tissue formation, and inflammatory cell infiltration (H&E stain, A, ×40, B, ×400).
Reference
-
1. Dikensoy O, Usalan C, Filiz A. Foreign body aspiration: clinical utility of flexible bronchoscopy. Postgrad Med J. 2002. 78:399–403.2. Sersar SI, Rizk WH, Bilal M, El Diasty MM, Eltantawy TA, Abdelhakam BB, et al. Inhaled foreign bodies: presentation, management and value of history and plain chest radiography in delayed presentation. Otolaryngol Head Neck Surg. 2006. 134:92–99.3. Applegate KE, Dardinger JT, Lieber ML, Herts BR, Davros WJ, Obuchowski NA, et al. Spiral CT scanning technique in the detection of aspiration of LEGO foreign bodies. Pediatr Radiol. 2001. 31:836–840.4. Mattie PA, Rawls HR, Cabasso I. Development of a radiopaque, autopolymerizing dental acrylic resin. J Prosthodont. 1994. 3:213–218.5. Barzo P, Molnar L, Minik K. Bronchial papillomas of various origins. Chest. 1987. 92:132–136.6. Greene JG, Tassin L, Saberi A. Endobronchial epithelial papilloma associated with a foreign body. Chest. 1990. 97:229–230.7. Berman DE, Wright ES, Edstrom HW. Endobronchial inflammatory polyp associated with a foreign body. Successful treatment with corticosteroids. Chest. 1984. 86:483–484.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Study of Foreign Body Aspiration in Infants and Children
- Clinical perspectives on 2-unit cantilevered resin-bonded fixed partial denture
- Chronic Obstructive Pneumonitis
- Prevention and management of foreign body ingestion and aspiration during the dental treatment
- CT Findings of Foreign Bodies in the Chest: A Pictorial Essay
