A Case of Esophago-mediatinal Fistula Due to Esophageal Tuberculosis
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Kosin University, Pusan, Korea. jangtw@ns.kosinmed.or.kr
- 21Department of Radiology, College of Medicine, Kosin University, Pusan, Korea.
Abstract
- The esophagus is a rate site for rarely involved site of tuberculosis. The most common cause of esophageal tuberculosis is secondary involvement from adjacent tuberculous lymphadenitis. Esophago-nodal or esophagobronchial fistulas may be formed when tuberculous lymph nodes erode the adjacent esophageal or bronchial wall. We report a patient diagnosed with esophageal tuberculosis, which was complicated by an esophago-mediastinal fistula, by endoscopy, sputum acid fast bacilli (AFB) stain, chest computed tomography (CT), and an esophagogram. The patient was treated with antituberculous agents and chest CT and endoscopy showed that the fistula had closed completely.
Keyword
MeSH Terms
Figure
-
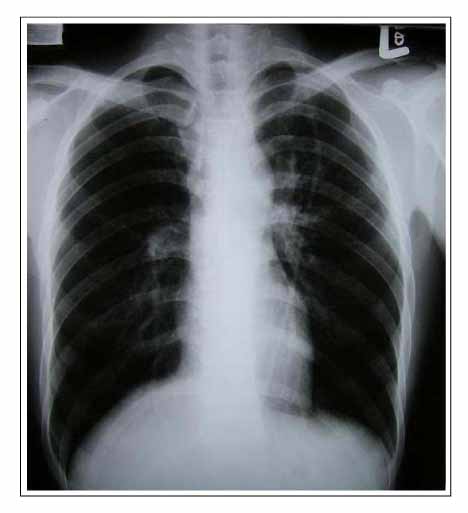
Figure 1 This radiographic study of chest shows multiple no-dular opacities in left upper zone. Perihilar engorgement is suspicious.
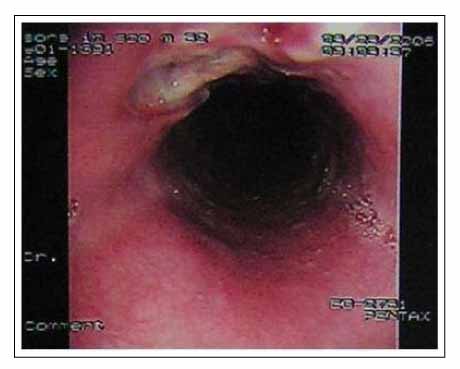
Figure 2 A 3 × 2 cm sized roundly deep ulce-rative lesion with fistular opening was noted at 33 cm site from upper incisor.

Figure 3 Esophagogram shows an irregular barium leakage outline the fistular in mid esophagus.

Figure 4 Contrast enhanced CT scan shows linear or oval gas collections in an enlarged left lower paratracheal lymph node. There is a communication between the esophagus and a mediastinal area of air attenuation and peripheral rim enhancement and calcified right lower lymph node.
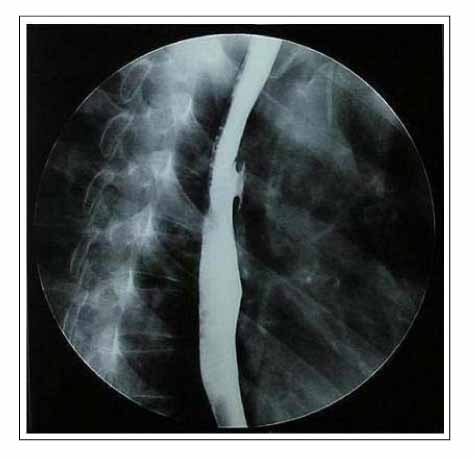
Figure 5 Shallow ulceration at left lateral wall of mid esophagus. No evidence of mediastinal leakage.
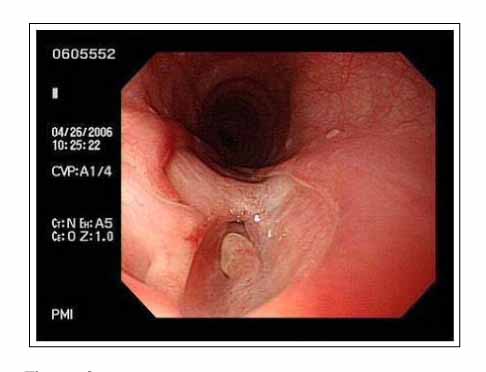
Figure 6 A shallow well demarcated defect with tiny fistulous opening was noted. Much improving state comparing with previous study.

Figure 7 Follow up contrast enhanced CT scan show no abnormal air collection in mediastinum.
Reference
-
1. Im JG, Kim JH, Han MC, Kim CW. Computed tomography of esophagomediastinal fistula in tuberculous mediastinal lymphadenitis. J Comput Assist Tomogr. 1990. 14:89–92.2. Williford ME, Thompson WM, Hamilton JD, Postlethwait RW. Esophageal tuberculosis: findings on barium swallow and computed tomography. Gastrointest Radiol. 1983. 8:119–122.3. Devarbhavi HC, Alvares JF, Radhikadevi M. Esophageal tuberculosis associated with esophagotracheal or esophagomediastinal fistula: report of 10 cases. Gastrointest Endosc. 2003. 57:588–592.4. Lockard LB. Esophageal tuberculosis: a critical review. Laryngoscope. 1913. 23:561–584.5. Fahmy AR, Guindi R, Farid A. Tuberculosis of the oesophagus. Thorax. 1969. 24:254–256.6. Gordon AH, Marshall JB. Esophageal tuberculosis: definitive diagnosis by endoscopy. Am J Gastroenterol. 1990. 85:174–177.7. Im JG, Song KS, Kang HS, Park JH, Yeon KM, Han MC, et al. Mediastinal tuberculous lymphadenitis: CT manifestations. Radiology. 1987. 164:115–119.8. Amorosa JK, Smith PR, Cohen JR, Ramsey C, Lyons HA. Tuberculous mediastinal lymphadenitis in the adult. Radiology. 1978. 126:365–368.9. Catinella FP, Kittle CF. Tuberculous esophagitis with aortic aneurysm fistula. Ann Thorac Surg. 1988. 45:87–88.10. Rubinstein BM, Pastrana T, Jacobson HG. Tuberculosis of the esophagus. Radiology. 1958. 70:401–403.11. Jain S, Kumar N, Das DK, Jain SK. Esophageal tuberculosis. Endoscopic cytology as a diagnostic tool. Acta Cytol. 1999. 43:1085–1090.12. Kochhar R, Sriram PV, Rajwanshi A, Gulati M, Kochhar S, Nagi B, et al. Transesophageal endoscopic fine-needle aspiration cytology in mediastinal tuberculosis. Gastrointest Endosc. 1999. 50:271–274.13. Lyons WS, Seremetis MG, deGuzman VC, Peabody JW Jr. Ruptures and perforations of the esophagus: the case for conservative supportive management. Ann Thorac Surg. 1978. 25:346–350.14. Lucaya J, Sole S, Badosa J, Manzanares R. Bronchial perforation and bronchoesophageal fistulas: tuberculous origin in children. AJR Am J Roentgenol. 1980. 135:525–528.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Esophago-Mediastinal Fistula Due to Tuberculous Mediastinal Lymphadenitis
- Endoscopic Treatment with a Cuffed Prosthesis for Malignant Esophago - Bronchial Fistula
- Congenital Tracheoesophageal Fistula in an Adult
- Endoscopic Treatment with a Cuffed Prosthesis for Esophago - tracheal Fistula without Esophageal Stricture in a Patient with Malignant Lymphoma
- A Case of Tuberculosis of the Esophagus and Duodenum Associated with Pulmonary Tuberculosis
