A Case of Therapeutic Keratoplasty Using Cryo-preservative Cornea in Candida albicans Keratitis
- Affiliations
-
- 1Department of Ophthalmology, Keimyung University School of Medicine, Daegu, Korea. junjonghwa@gmail.com
- KMID: 2317582
- DOI: http://doi.org/10.3341/jkos.2016.57.7.1170
Abstract
- PURPOSE
To report a case treated with therapeutic keratoplasty using a cryo-preserved cornea in a patient with Candida albicans keratitis.
CASE SUMMARY
A 77-year-old female visited our clinic because of left ocular pain and visual disturbance for 3 days. Microscopic slit lamp examination revealed a 1.2 mm sized round corneal epithelial defect with deep stromal infiltration, brownish pigmentation and signs of inflammation with cyclitic membranes in the anterior chamber. On suspicion of Candida keratitis, we performed penetrating keratoplasty using a cryo-preserved donor cornea in Optisol-GS® (Bausch & Lomb, Irvine, CA, USA) solution with excision of the infected iris and colony of the anterior chamber. After the procedure, injection of intravitreal or intracameral amphotericin B and voriconazole were administered alternately. At 2 weeks after the second surgery, infection signs disappeared. At the follow-up in the outpatient clinic, signs of infection were not observed.
CONCLUSIONS
Therapeutic keratoplasty using a cryo-preserved donor cornea can be an immediate and effective therapeutic strategy for Candida albicans keratitis.
MeSH Terms
Figure
-

Figure 1. Anterior segment photographs of the initial ophthalmic examination. (A) A 1.2 mm-sized thick and deep stromal infiltration with central brownish pigmentation (arrow). (B) Fluorescein staining revealed a round and well demarcated epithelial defect (arrowhead).
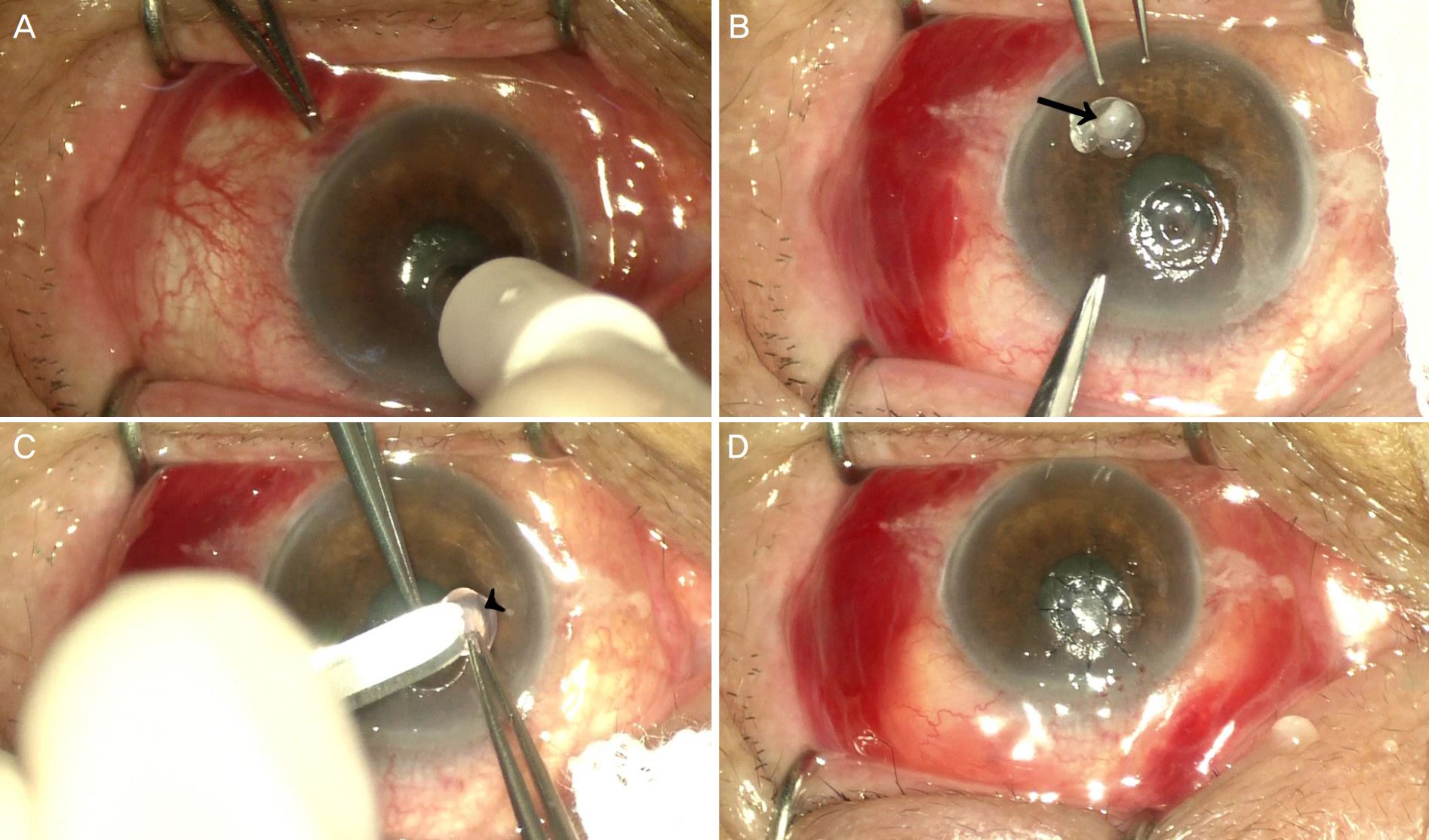
Figure 2. The serial surgical steps of therapeutic lamellar keratoplasty using a cryopreserved cornea. (A) Infected cornea was trephined with skin biopsy punch 3.0 mm in diameter. (B) Additionally, the infected cornea and visible inflamed tissues were removed. The dissected lesion is shown (arrow). (C) Lamellar dissection of cryopreserved cornea was performed using a crescent corneal blade (arrowhead). (D) A lamellar graft of the same diameter was positioned and sutured using 10–0 nylon.

Figure 3. The serial surgical step of therapeutic penetrating keratoplasty using a cryopreserved cornea. (A) Previous lamellar graft was infected and colonies of the Candida species spread to the iris and anterior surface of the crystalline lens. (B) The previous lamellar graft was trephined with skin biopsy punch 4.0 mm in diameter. (C) Status after full thickness keratectomy. Coagulum at anterior chamber (arrow) was observed. (D) Removal of coagulum using vannas scissors (arrowhead). (E) The full thickness cryopreserved corneal graft was obtained using the same-sized skin biopsy punch and sutured with 10–0 nylon. (F) A full thickness graft of the same diameter was positioned and sutured using 10–0 nylon.

Figure 4. Postoperative slitlamp photograph and anterior segment optical coherence tomography (OCT). (A) After 2 months, the corneal graft was well attached and no signs of a recurring infection were observed (arrowhead). (B) Anterior segment OCT at 2 months after the operation shows well attached corneal graft (between arrows) and slightly swollen epithelium. OS = oculus sinister.
Reference
-
References
1. Cheikhrouhou F, Makni F, Neji S, et al. Epidemiological profile of fungal keratitis in Sfax (Tunisia). J Mycol Med. 2014; 24:308–12.
Article2. Sun RL, Jones DB, Wilhelmus KR. Clinical characteristics and outcome of Candida keratitis. Am J Ophthalmol. 2007; 143:1043–5.
Article3. Spierer O, Dugar J, Miller D, O'Brien TP. Comparative antifungal susceptibility analysis of Candida albicans versus non-albicans Candida corneal isolates. Cornea. 2015; 34:576–9.
Article4. Sengupta J, Khetan A, Saha S, et al. Candida keratitis: emerging problem in India. Cornea. 2012; 31:371–5.5. Yao YF, Zhang YM, Zhou P, et al. Therapeutic penetrating abdominal in severe fungal keratitis using cryopreserved donor corneas. Br J Ophthalmol. 2003; 87:543–7.6. Cristol SM, Alfonso EC, Guildford JH, et al. Results of large abdominal keratoplasty in microbial keratitis. Cornea. 1996; 15:571–6.7. Ang M, Mehta JS, Sng CC, et al. Indications, outcomes, and risk factors for failure in tectonic keratoplasty. Ophthalmology. 2012; 119:1311–9.
Article8. Shimazaki J, Shimmura S, Ishioka M, Tsubota K. Randomized clinical trial of deep lamellar keratoplasty vs penetrating keratoplasty. Am J Ophthalmol. 2002; 134:159–65.9. Ilango B. Comparative cohort study of the outcomes of deep abdominal keratoplasty and penetrating keratoplasty for keratoconus. Eye (Lond). 2007; 21:447. author reply 447.10. Fogla R, Padmanabhan P. Results of deep lamellar keratoplasty abdominal the big-bubble technique in patients with keratoconus. Am J Ophthalmol. 2006; 141:254–9.11. Soong HK, Farjo AA, Katz D, et al. Lamellar corneal patch grafts in the management of corneal melting. Cornea. 2000; 19:126–34.
Article12. Lalitha P, Prajna NV, Kabra A, et al. Risk factors for treatment abdominal in fungal keratitis. Ophthalmology. 2006; 113:526–30.13. Xie L, Dong X, Shi W. Treatment of fungal keratitis by penetrating keratoplasty. Br J Ophthalmol. 2001; 85:1070–4.
Article14. Killingsworth DW, Stern GA, Driebe WT, et al. Results of abdominal penetrating keratoplasty. Ophthalmology. 1993; 100:534–41.15. Lim LS, Arundhati A, Tan DT. Sequential therapeutic penetrating keratoplasty with cryopreserved and fresh corneal tissue for severe infectious keratitis: a case-control study. Cornea. 2011; 30:739–43.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Efficacy of Fluconazole in The Treatment of Candida albicans Keratitis in Rabbits
- Excimer Laser Phototherapeutic Keratectomy for Experimental Fungal Keratitis
- Development of Keratitis by Soft Contact Lenses Contaminated with Candida albicans
- The Effect of Ketoconazole in the Treatment of Candida albicans Keratitis in Rabbits
- A Report of Five Cases of Mixed Candida and Bacterial Keratitis
