J Korean Ophthalmol Soc.
2016 Jul;57(7):1134-1138. 10.3341/jkos.2016.57.7.1134.
Unilateral Lateral Rectus Muscle Advancement Surgery Based on One-fourth of the Angle of Consecutive Esotropia
- Affiliations
-
- 1Department of Ophthalmology, Haeundae Paik Hospital, Inje University College of Medicine, Busan, Korea. kris9352@hanmail.net
- KMID: 2317575
- DOI: http://doi.org/10.3341/jkos.2016.57.7.1134
Abstract
- PURPOSE
To evaluate the efficacy of unilateral lateral rectus muscle advancement surgery based on one-fourth of the angle of consecutive esotropia within 25 prism diopters (PD) which occurred after bilateral lateral rectus muscle recession for intermittent exotropia.
METHODS
Medical records of 11 patients who underwent unilateral lateral rectus muscle advancement for consecutive esotropia from 2011 to 2014 and who were observed for at least 6 months after surgery were retrospectively reviewed. The change in the angle of deviation before and after consecutive esotropia surgery, success rate, and surgical effect were evaluated.
RESULTS
Preoperative esodeviation was -19.6 ± 4.7 PD at distance and -16.5 ± 7.4 PD at near. Unilateral lateral rectus muscle advancement surgeries were performed based on one-fourth of the angle of consecutive esotropia and the mean surgical amount was 4.8 ± 1.1 mm. Of the total 11 patients, 10 patients (91%) recovered to orthotropia or exodeviation within 8 PD. One patient had a recurrence of esotropia at postoperative 3 months, but the patient recovered to orthotropia at postoperative 12 months with alternative patch treatment and a prism glass prescription. The surgical effect of unilateral lateral rectus muscle advancement was 3.3 ± 0.7 PD/mm at postoperative 1 day, 3.7 ± 0.6 PD/mm at postoperative 1 week, and 3.8 ± 0.7 PD/mm at postoperative 6 months.
CONCLUSIONS
Unilateral lateral rectus muscle advancement surgery based on one-fourth of the angle of consecutive esotropia within 25 PD was successful in all 11 cases. The surgical effect was significantly greater in unilateral lateral rectus muscle advancement than in primary lateral rectus muscle recession. Thus, reduction in the amount of surgery should be considered carefully in unilateral lateral rectus muscle advancement for consecutive esotropia.
MeSH Terms
Figure
-
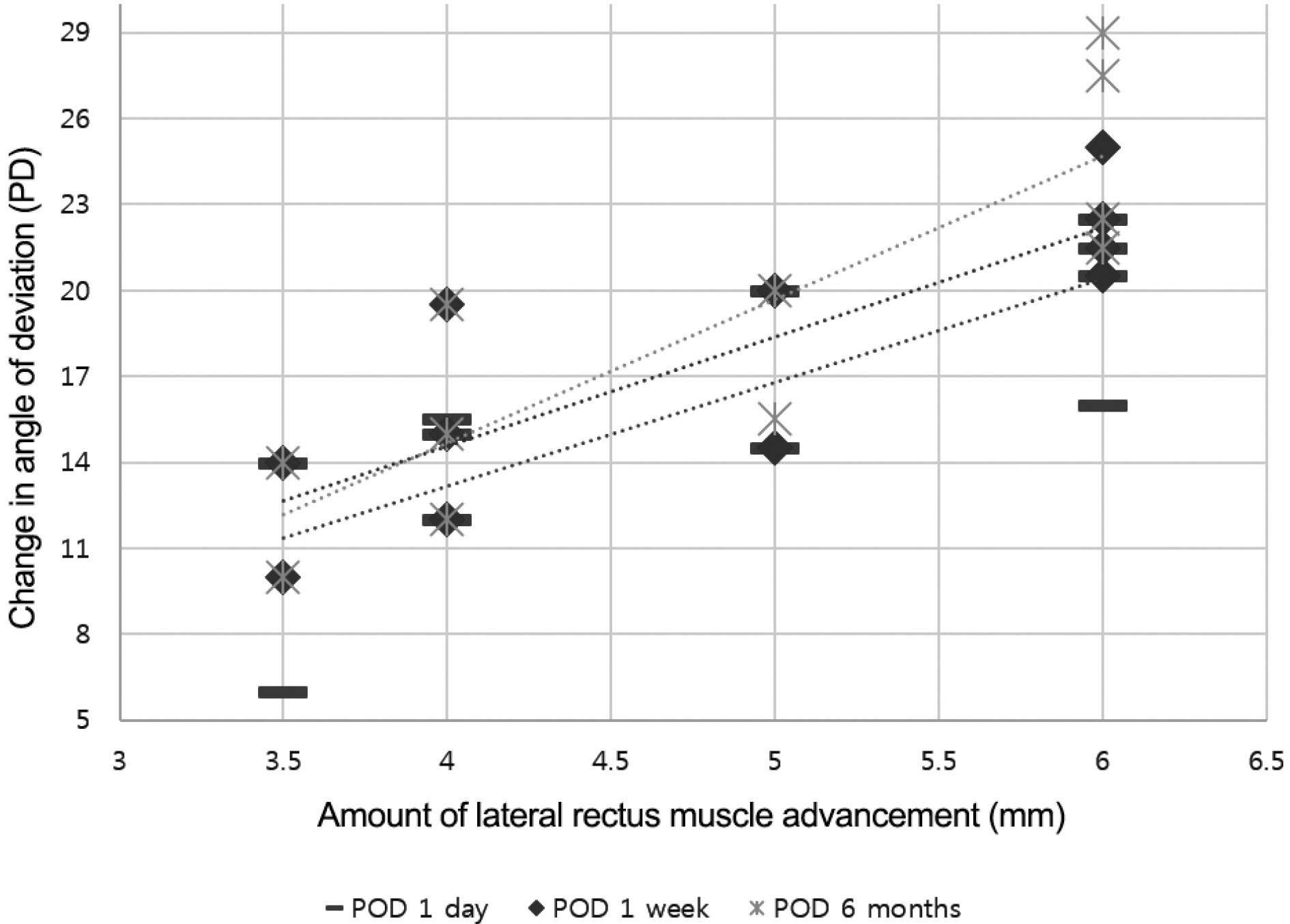
Figure 1. Linear regression analysis shows positive correlation between the amount of lateral rectus muscle advancement (x) and change in angle of deviation (y) at postoperative 1 day (R2= 0.63, p = 0.004), 1 week (R2 = 0.70, p =0.001) and 6 months (R2 = 0.74, p =0.001). There was significant difference. POD = postoperative day.
Reference
-
References
1. Cooper EL. The surgical management of secondary exotropia. Trans Am Acad Ophthalmol Otolaryngol. 1961; 65:595–608.2. Lee JH, Lee SY, Lee YC. The effect of lateral rectus muscle abdominal in consecutive esotropia after bilateral rectus muscle recession. J Korean Ophthalmol Soc. 2008; 49:1801–6.3. Kim JS, Son KH. The effect of advancement of the lateral rectus muscle on the consecutive esotropia. J Korean Ophthalmol Soc. 1995; 36:1784–9.4. Shin KH, Wi JM, Paik HJ. The long-term outcome of lateral rectus advancement in patients with consecutive esotropia following abdominal lateral rectus recession for intermittent exotropia. J Korean Ophthalmol Soc. 2014; 55:1180–6.5. Adamopoulou C, Rao RC. Surgical correction of consecutive abdominal with unilateral medial rectus recession. J Pediatr Ophthalmol Strabismus. 2015; 52:343–7.6. Hardesty HH. Treatment of overcorrected intermittent exotropia. Am J Ophthalmol. 1968; 66:80–6.
Article7. Parks MM. Atlas of strabismus surgery. Philadelphia: Harper and Row Publishing;1983.8. Kim BH, Suh SY, Kim JH, et al. Surgical dose-effect relationship in single muscle advancement in the treatment of consecutive strabismus. J Pediatr Ophthalmol Strabismus. 2014; 51:93–9.
Article9. Hwang KY, Lee SY, Lee YC. Change of strabismus angle and abdominal after unilateral or bilateral lateral rectus recession in exotropia. J Korean Ophthalmol Soc. 2011; 52:60–6.10. Lee SN, Shin DB, Xu YG, Min BM. Effect of unilateral lateral abdominal recession for intermittent exotropia under 25 PD. J Korean Ophthalmol Soc. 2002; 43:1469–73.11. Nelson LB, Bacal DA, Burke MJ. An alternative approach to the surgical management of exotropia-the unilateral lateral rectus recession. J Pediatr Ophthalmol Strabismus. 1992; 29:357–60.
Article12. Wilson ME. “Tying the knot”-surgical choices in esotropia: when? how much? how many? Am Orthopt J. 1996; 46:65–72.
Article13. Cho YA, Ryu WY. The advancement of the medial rectus muscle for consecutive exotropia. Can J Ophthalmol. 2013; 48:300–6.
Article14. Chatzistefanou KI, Droutsas KD, Chimonidou E. Reversal of abdominal medial rectus recession and lateral rectus resection for the correction of consecutive exotropia. Br J Ophthalmol. 2009; 93:742–6.15. Jampolsky A. Surgical correction of overcorrections in strabismus. Am Orthopt J. 1976; 26:14–9.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Lateral Rectus Muscle Advancement in Consecutive Esotropia After Bilateral Rectus Muscle Recession
- The Effect of Advancement of the Lateral Rectus Muscle on the Consecutive Esotropia
- Clinical Evaluation on the Consecutive Esotropia after Exotropia Surgery
- Consecutive Esotropia after Surgical Correction of Intermittent Exotropia
- The Long-Term Outcome of Lateral Rectus Advancement in Patients with Consecutive Esotropia Following Bilateral Lateral Rectus Recession for Intermittent Exotropia
