Pediatr Allergy Respir Dis.
2011 Jun;21(2):131-136.
A Case of Laryngeal Neurofibroma with Sleep Obstructive Apnea
- Affiliations
-
- 1Department of Pediatrics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. sjhong@amc.seoul.kr
- 2Childhood Asthma Atopy Center, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Abstract
- Most patients with neurofibromas suffer from neurofibromatosis type 1 (von Recklinghausen's disease), which is characterized by cafe-au-lait spots and cutaneous neurofibromas. Neurofibromas in the laryngeal area are extremely rare. Most patients with a laryngeal neurofibroma present with dyspnea, dysphagia, stridor, or hoarseness, depending on the location and size of the tumor. We present a case of a laryngeal neurofibroma in a boy with neurofibromatosis type 1. A 30-month-old boy with neurofibromatosis presented to our hospital with respiratory difficulty and obstructive sleep apnea. Magnetic resonance imaging demonstrated a round mass over the left carotid space, and its location made surgical resection impossible. Hence, tracheostomy was performed to maintain airway patency. The patient's symptoms improved after tracheostomy. Long-term follow-up is essential owing to the possibility of recurrence. The patient has thus far shown no obstructive airway symptoms for one year after closure of the tracheostomy.
MeSH Terms
Figure
-
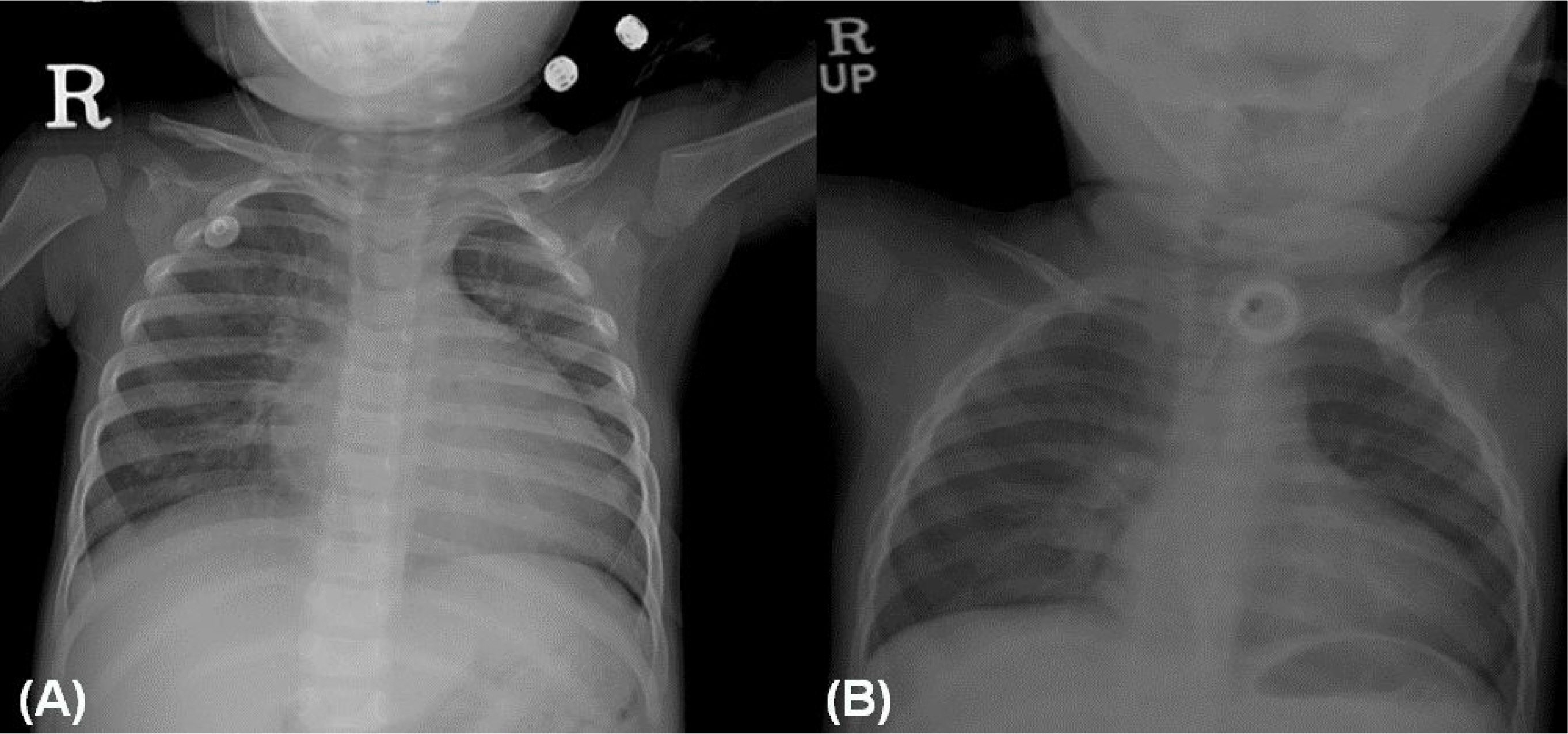
Fig. 1. Chest radiograph showed (A) cardiomegaly with pulmonary congestion before tracheostomy and (B) improved cardiomegaly after tracheostomy.
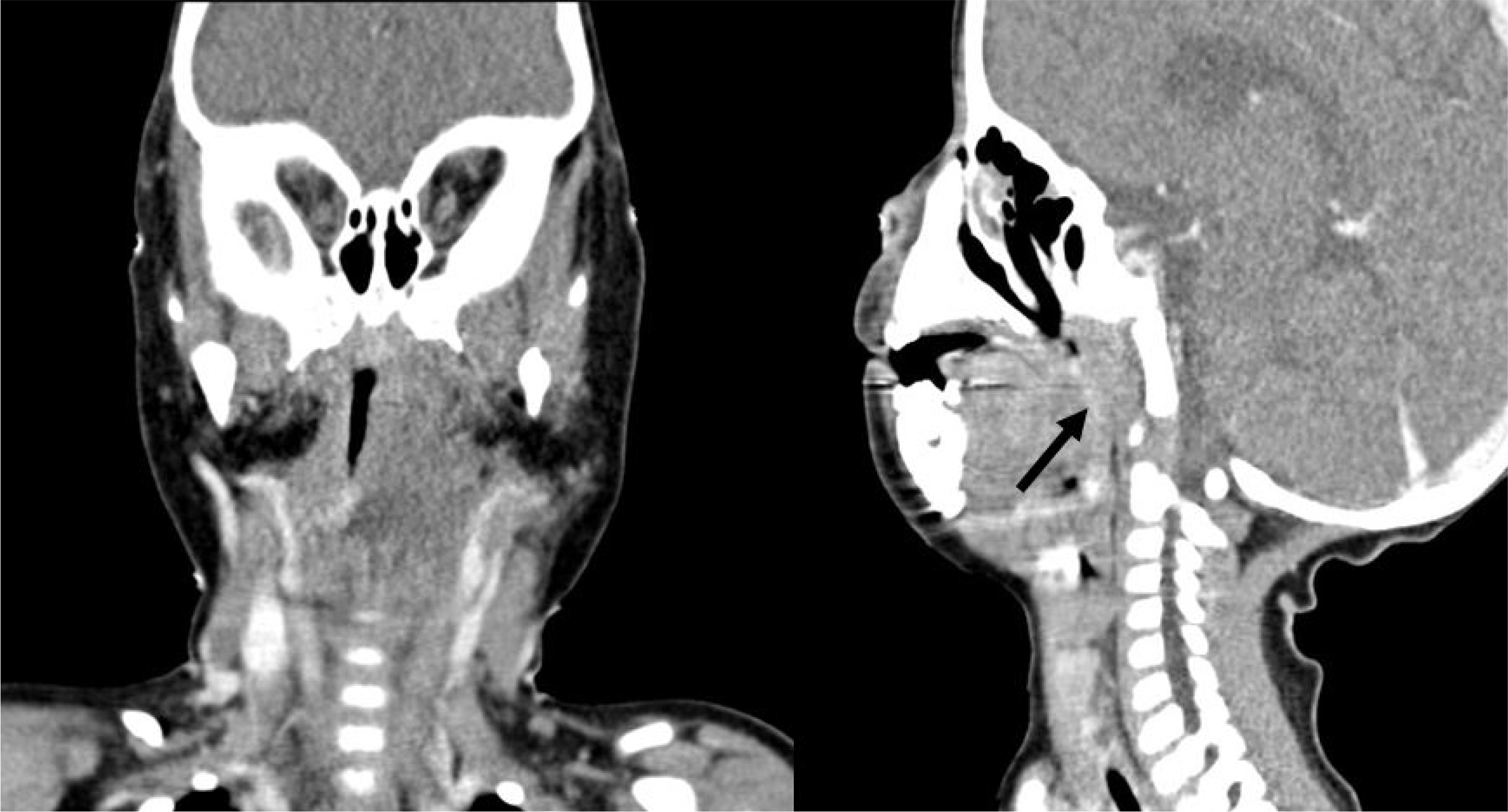
Fig. 2. Neck computed tomography scan showed asymmetric obliteration of nasopharynx and larynx secondary to ill-defined hypodense mass-like lesion.
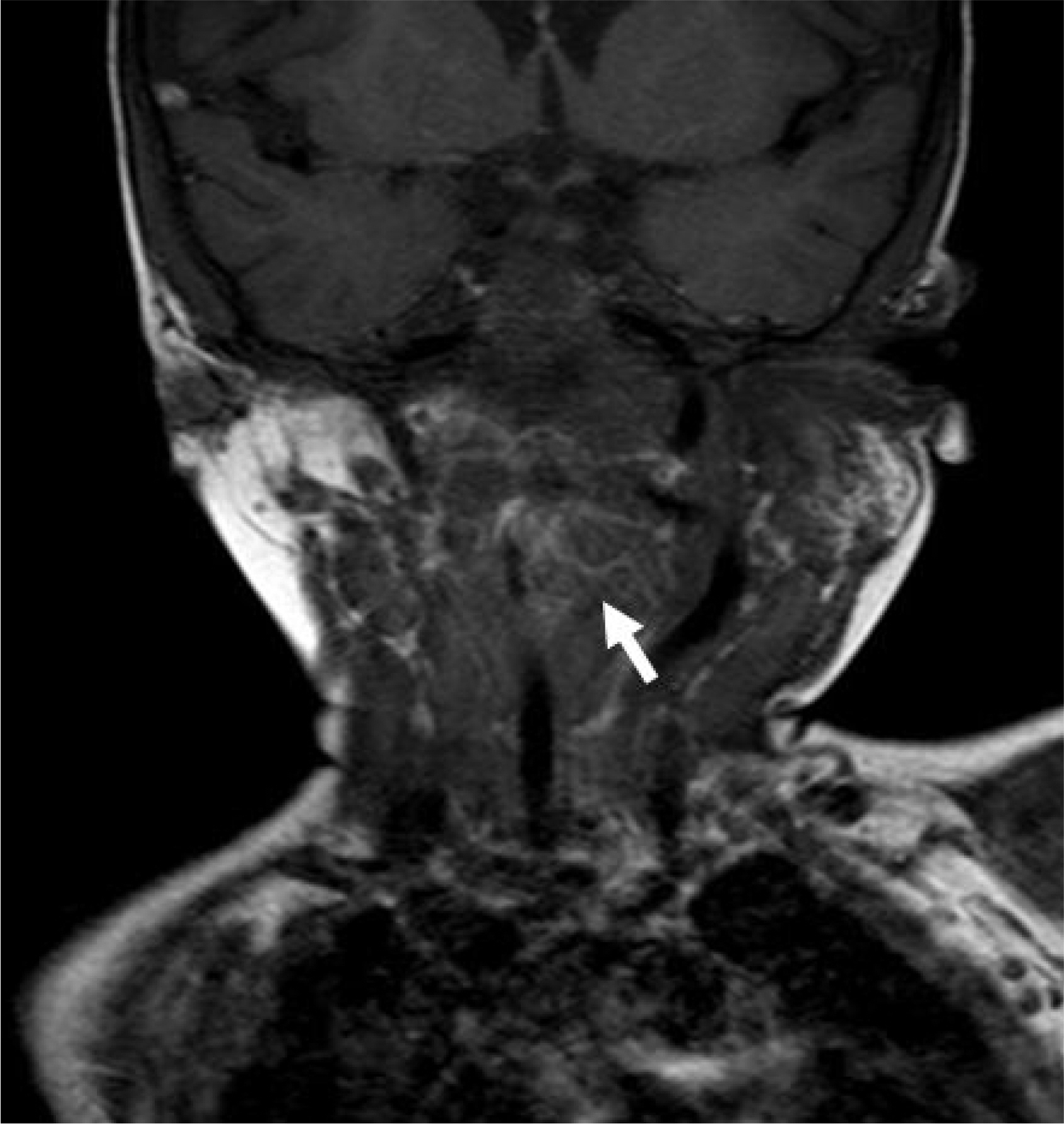
Fig. 3. An axial magnetic resonance imaging revealed about 4 cm sized, hyperintense, minimally enhancing, multinodular and infiltrative mass involving left parapharyngeal and left carotid space.

Fig. 4. Bronchoscopic examination showed omega shape edema in the supraglottic area adjacent to the epiglottis.
Reference
-
References
1. Sabol Z, Kipke-Sabol L. Neurofibromatosis type 1 (von Recklinghausen's disease or peripheral neurofibromatosis): from phenotype to gene. Lijec Vjesn. 2005; 127:303–11.2. Evans GR, Lloyd SK, Ramsden RT. Neurofibromatosis type 2. Adv Otorhinolaryngol. 2011; 70:91–8.
Article3. Boudewyns A, Claes J, Van de Heyning P. Clinical practice: an approach to stridor in infants and children. Eur J Pediatr. 2010; 169:135–41.4. Chen YW, Fang TJ, Li HY. A solitary laryngeal neurofibroma ina pediatric patient. Chang Gung Med J. 2004; 27:930–3.5. Shah KN. The diagnostic and clinical significance of café-au-lait macules. Pediatr Clin North Am. 2010; 57:1131–53.
Article6. Polgár N, Komlósi K, Hadzsiev K, Illés T, Me-legh B. Molecular genetic diagnosis of neurofibromatosis type I. Orv Hetil. 2011; 152:415–9.
Article7. Suchanek E. Neurinom des kehlkopfeinganges. Monatsschr Orhenheilkd Laryngo-Rhinol. 1925; 50:613–7.8. Willcox TO Jr, Rosenberg SI, Handler SD. Laryngeal involvement in neurofibromatosis. Ear Nose Throat J. 1993; 72:811–2. 815.
Article9. Masip MJ, Esteban E, Alberto C, Menor F, Cortina H. Laryngeal involvement in pediatric neurofibromatosis: a case report and review of the literature. Pediatr Radiol. 1996; 26:488–92.
Article10. Powell S, Kubba H, O'Brien C, Tremlett M. Paediatric obstructive sleep apnoea. BMJ. 2010; 340:c1918.11. Marcus CL, Carroll JL, Koerner CB, Hamer A, Lutz J, Loughlin GM. Determinants of growth in children with the obstructive sleep apnea syndrome. J Pediatr. 1994; 125:556–62.
Article12. Bland RM, Bulgarelli S, Ventham JC, Jackson D, Reilly JJ, Paton JY. Total energy expenditure in children with obstructive sleep apnoea syndrome. Eur Respir J. 2001; 18:164–9.
Article13. Amin RS, Kimball TR, Bean JA, Jeffries JL, Willging JP, Cotton RT, et al. Left ventricular hypertrophy and abnormal ventricular geometry in children and adolescents with obstructive sleep apnea. Am J Respir Crit Care Med. 2002; 165:1395–9.
Article14. Enright PL, Goodwin JL, Sherrill DL, Quan JR, Quan SF. Tucson Children's Assessment of Sleep Apnea study. Blood pressure elevation associated with sleep-related breathing disorder in a community sample of white and Hispanic children: the Tucson Children's Assessment of Sleep Apnea study. Arch Pediatr Adolesc Med. 2003; 157:901–4.15. Kraiczi H, Caidahl K, Samuelsson A, Peker Y, Hedner J. Impairment of vascular endothelial function and left ventricular filling: association with the severity of apnea-induced hypoxemia during sleep. Chest. 2001; 119:1085–91.16. Needle MN, Cnaan A, Dattilo J, Chatten J, Phillips PC, Shochat S, et al. Prognostic signs in the surgical management of plexiform neurofibroma: the Children's Hospital of Philadelphia experience, 1974–1994. J Pediatr. 1997; 131:678–82.
Article17. Sidman J, Wood RE, Poole M, Postma DS. Management of plexiform neurofibroma of the larynx. Ann Otol Rhinol Laryngol. 1987; 96(1 Pt 1):53–5.
Article18. Rahbar R, Litrovnik BG, Vargas SO, Robson CD, Nuss RC, Irons MB, et al. The biology and management of laryngeal neurofibroma. Arch Otolaryngol Head Neck Surg. 2004; 130:1400–6.
Article19. Ransom ER, Yoon C, Manolidis S. Single stage near total resection of massive pediatric head and neck plexiform neurofibromas. Int J Pediatr Otorhinolaryngol. 2006; 70:1055–61.
Article
