Technique of fetal echocardiography
- Affiliations
-
- 1Department of Obstetrics and Gynecology, University of Ulsan College of Medicine, Asan Medical Center, Seoul, Korea. hswon@amc.seoul.kr
Abstract
- Congenital heart disease is the most common abnormality in the human fetus. Fetal echocardiography has been used to detect the majority of cardiac defects, and it is now part of the routine screening method for fetal evaluation. In this article, we present standard ultrasonographic views of the normal fetal heart obtained during the second trimester, first-trimester fetal echocardiography findings, and a modified myocardial performance index.
MeSH Terms
Figure
-
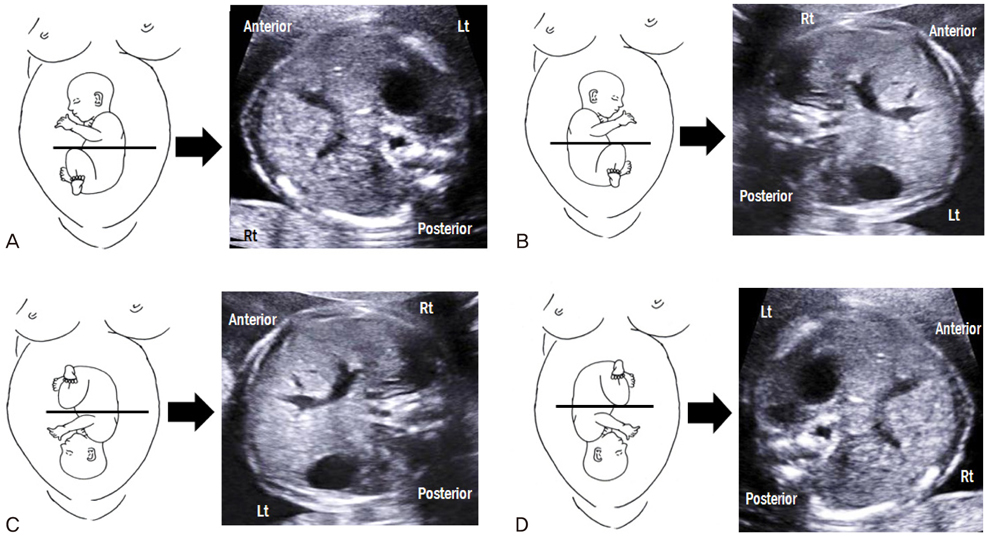
Fig. 1 Schematic images and transverse abdominal views of fetuses with breech and vertex presentations. (A) Breech presentation with fetal occiput on the maternal left side. (B) Breech presentation with fetal occiput on the maternal right side. (C) Vertex presentation with fetal occiput on the maternal left side. (D) Vertex presentation with fetal occiput on the maternal right side.
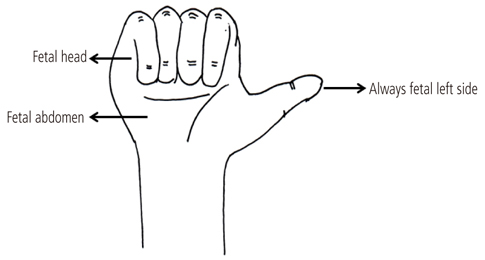
Fig. 2 Right-hand rule of thumb for transabdominal scanning. The palm of the right hand corresponds to the fetal abdomen, the dorsal side of the forearm to the fetal back, and the fist to the fetal head. The direction of the thumb always corresponds to the left side of the fetus.
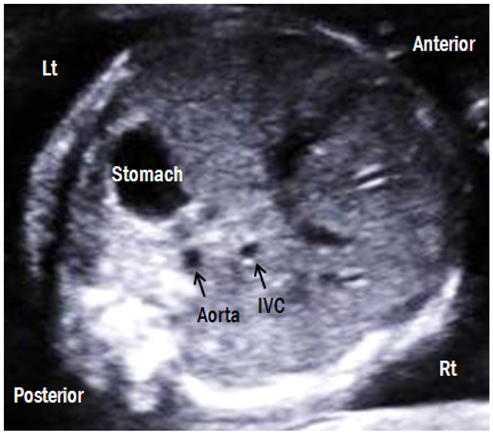
Fig. 3 Transverse abdominal view. The fetal stomach is on the left side and liver is on the right side. The descending aorta is posterior-left located and the IVC is anterior-right located. Lt, left; Rt, right; IVC, inferior vena cava.
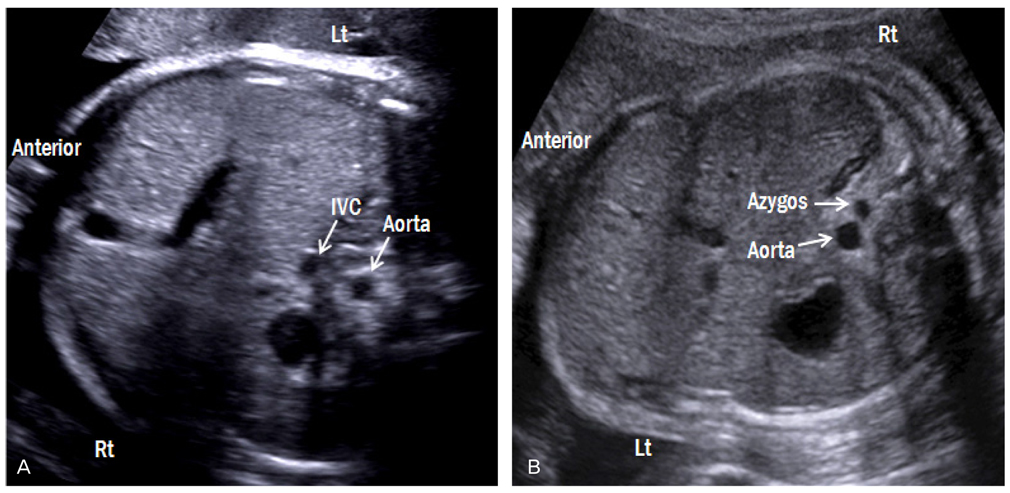
Fig. 4 Transverse abdominal views of both forms of heterotaxy syndrome. (A) Fetus with right atrial isomerism (breech presentation) shows juxtaposition of the aorta and IVC on either left side of the spine. The right-sided stomach and the midline liver are also shown. (B) Fetus with left atrial isomerism (vertex presentation) shows invisible IVC with dilated azygos vein, suggestive of an interrupted IVC with azygos vein continuation. Lt, left; Rt, right; IVC, inferior vena cava.
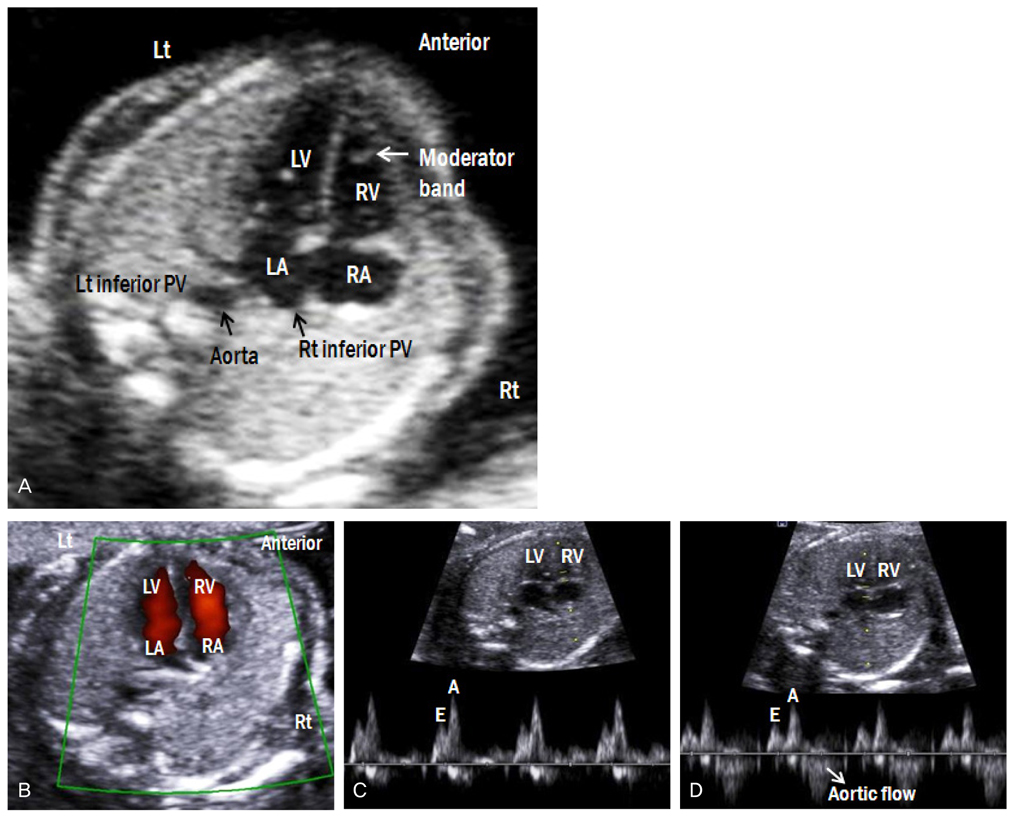
Fig. 5 (A) Apical four-chamber view of the fetal heart. (B) Color Doppler image shows forward flow from both atria to both ventricles. (C) Doppler waveforms of tricuspid and (D) mitral valves show a biphasic pattern. The E wave corresponds to early ventricular filing of the diastole, and the A wave corresponds to active ventricular filling of the diastole (atrial contraction). (D) Because of the continuity between mitral and aortic valves, the Doppler waveform at the mitral valve shows aortic outflow. Lt, left; Rt, right; LA, left atrium; RA, right A atrium; LV, left ventricle; RV, right ventricle; PV, pulmonary vein.
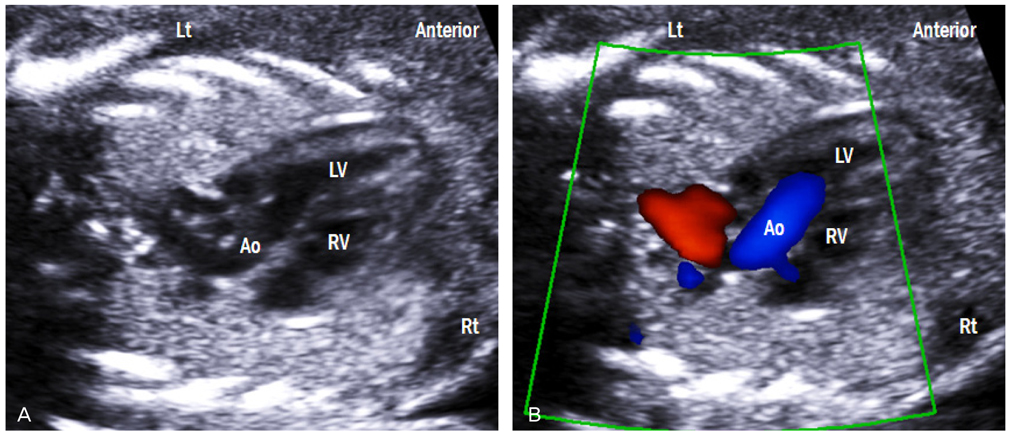
Fig. 6 Left ventricular outflow tract view. (A) This view shows the ventriculoarterial connection and intact ventricular septum. (B) Color Doppler across the aortic valve shows laminar flow and no turbulence in systole. Lt, left; Rt, right; LV, left ventricle; RV, right ventricle; Ao, aorta.
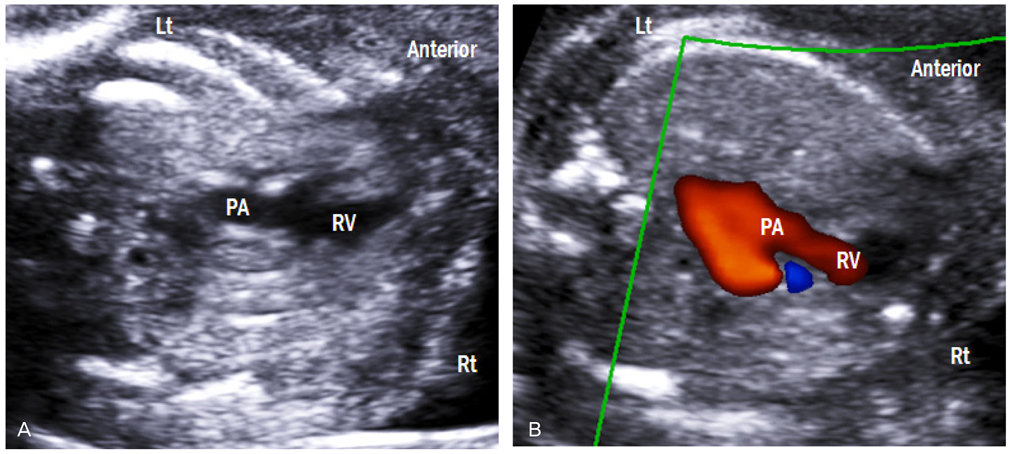
Fig. 7 Right ventricular outflow tract view. (A) This view shows the right ventriculoarterial connection. (B) Color Doppler image demonstrates laminar flow across the pulmonary valve. Lt, left; Rt, right; RV, right ventricle; PA, pulmonary artery.
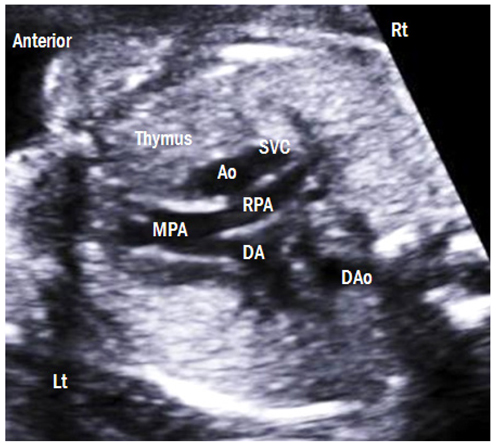
Fig. 8 Three-vessel view. The main pulmonary artery, ascending aorta, and superior vena cava are arranged in a straight line from the left anterior to the right posterior aspect. The pulmonary artery is the largest in size, followed by the ascending aorta and the superior vena cava. The thymus is clearly visible anterior to the three vessels. Lt, left; Rt, right; MPA, main pulmonary artery; RPA, right pulmonary artery; DA, ductus arteriosus; Ao, aorta; SVC, superior vena cava; DAo, descending aorta.
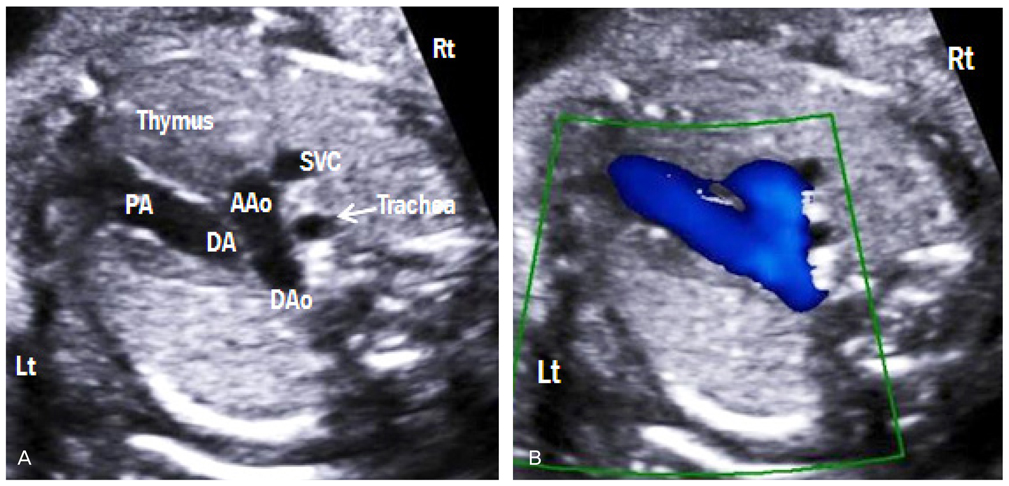
Fig. 9 Three-vessel-trachea view. (A) This view demonstrates a V-shaped confluence of aortic and ductal arches at the descending aorta. (B) The trachea is located to the right side of the aorta. Color Doppler shows the same direction of blood flow in both arches. Lt, left; Rt, right; PA, pulmonary artery; DA, ductus arteriosus; AAo, ascending aorta; DAo, descending aorta; SVC, superior vena cava.
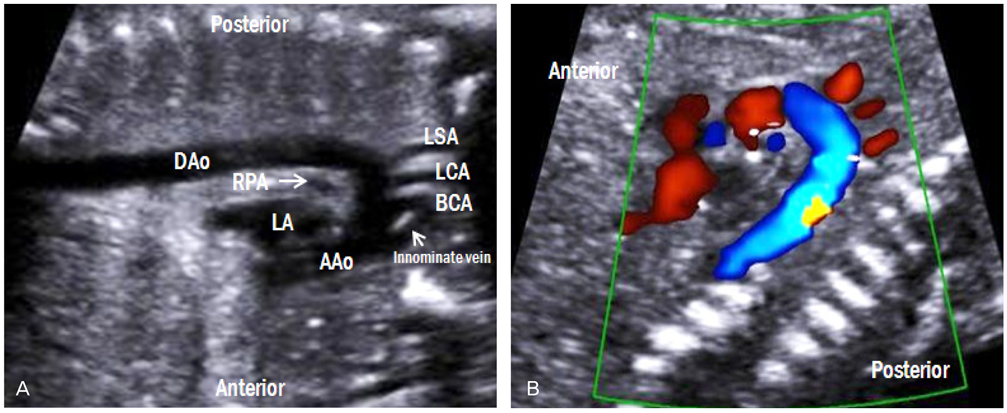
Fig. 10 Aortic arch view. (A) A 'candy cane-like' aorta gives rise to the three arterial branches, namely, the brachiocephalic, left common carotid, and left subclavian arteries. (B) These three branches are also visible by color Doppler imaging. LA, left atrium; RPA, right pulmonary artery; AAo, ascending aorta; DAo, descending aorta; BCA, brachiocephalic artery; LCA, left common carotid artery; LSA, left subclavian artery.
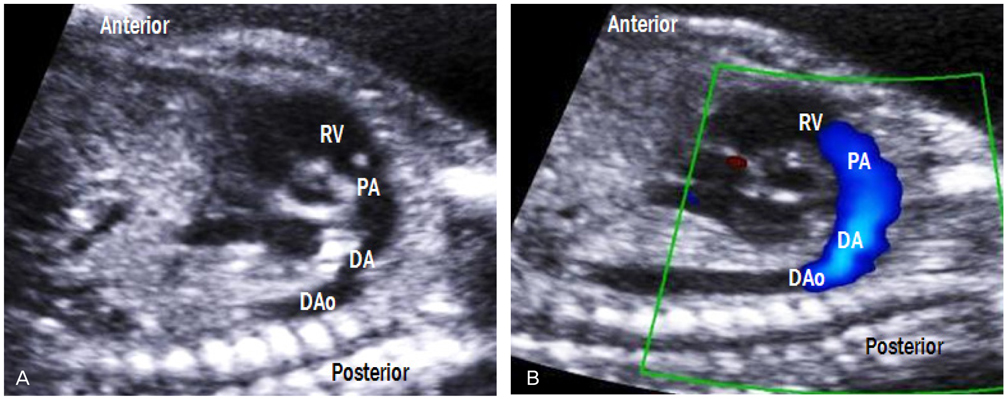
Fig. 11 Ductal arch view. (A) The ductus arteriosus connects the main pulmonary artery to the DAo, forming hockey stick-shaped arch. (B) Laminar flow across the pulmonary valve is also shown. RV, right ventricle; PA, pulmonary artery; DA, ductus arteriosus; DAo, descending aorta.
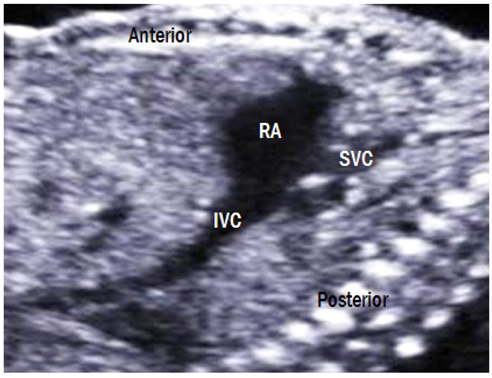
Fig. 12 Bicaval view. The SVC and IVC drain into the posterior aspect of the right atrium. The IVC is widened as it enters the right atrium because of interflow from the ductus venosus and hepatic veins. RA, right atrium; IVC, inferior vena cava; SVC, superior vena cava.
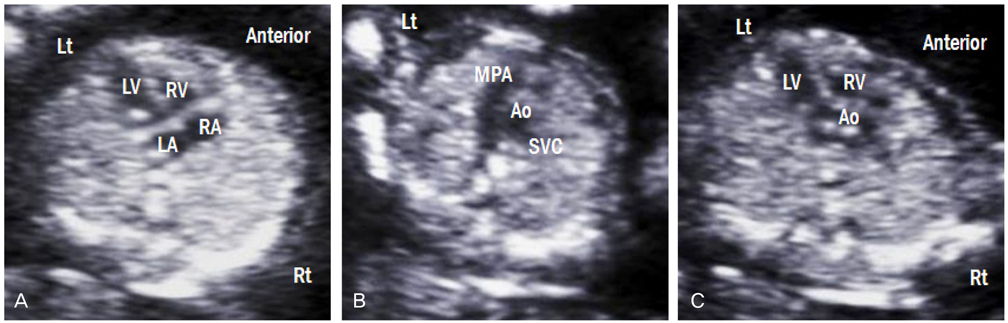
Fig. 13 Ultrasonographic images of fetuses with a normal heart at 13 weeks of gestation. (A) Four-chamber view. (B) Three-vessel view. (C) Left ventricular outflow tract view. Lt, left; Rt, right; LA, left atrium; RA, right atrium; LV, left ventricle; RV, right ventricle; MPA, main pulmonary artery; Ao, aorta; SVC, superior vena cava.

Fig. 14 Measurement of the fetal modified myocardial performance index. Each cursor should be placed at the beginning of each valve click, and the modified myocardial performance index is calculated as the sum of ICT and IRT divided by ejection time. AV, aortic valve; MV, mitral valve; ICT, isovolumetric contraction time; IRT, isovolumetric relaxation time; ET, ejection time.
Reference
-
1. Hoffman JI, Christianson R. Congenital heart disease in a cohort of 19,502 births with long-term follow-up. Am J Cardiol. 1978. 42:641–647.2. Bronshtein M, Gover A, Zimmer EZ. Sonographic definition of the fetal situs. Obstet Gynecol. 2002. 99:1129–1130.3. Allan LD. A practical approach to fetal heart scanning. Semin Perinatol. 2000. 24:324–330.4. Paladini D, Chita SK, Allan LD. Prenatal measurement of cardiothoracic ratio in evaluation of heart disease. Arch Dis Child. 1990. 65:20–23.5. Chaoui R, Bollmann R, Goldner B, Heling KS, Tennstedt C. Fetal cardiomegaly: echocardiographic findings and outcome in 19 cases. Fetal Diagn Ther. 1994. 9:92–104.6. Comstock CH. Normal fetal heart axis and position. Obstet Gynecol. 1987. 70:255–259.7. Allan L. Technique of fetal echocardiography. Pediatr Cardiol. 2004. 25:223–233.8. Jung E, Won HS, Lee PR, Kim A, Park IS. Clinical implication of isolated right dominant heart in the fetus. Prenat Diagn. 2007. 27:695–698.9. Rizzo G, Arduini D, Romanini C. Doppler echocardiographic assessment of fetal cardiac function. Ultrasound Obstet Gynecol. 1992. 2:434–445.10. Allan LD, Chita SK, Al-Ghazali W, Crawford DC, Tynan M. Doppler echocardiographic evaluation of the normal human fetal heart. Br Heart J. 1987. 57:528–533.11. Reed KL, Anderson CF, Shenker L. Fetal pulmonary artery and aorta: two-dimensional Doppler echocardiography. Obstet Gynecol. 1987. 69:175–178.12. Yoo SJ, Lee YH, Kim ES, Ryu HM, Kim MY, Choi HK, et al. Three-vessel view of the fetal upper mediastinum: an easy means of detecting abnormalities of the ventricular outflow tracts and great arteries during obstetric screening. Ultrasound Obstet Gynecol. 1997. 9:173–182.13. Pasquini L, Mellander M, Seale A, Matsui H, Roughton M, Ho SY, et al. Z-scores of the fetal aortic isthmus and duct: an aid to assessing arch hypoplasia. Ultrasound Obstet Gynecol. 2007. 29:628–633.14. Abuhamad A, Chaoui R. Abuhamad A, Chaoui R, editors. The great vessels. A practical guide to fetal echocardiography. 2010. 2nd ed. Philadelphia (PA): Lippincott Williams & Wilkins;60–76.15. Gembruch U, Knopfle G, Chatterjee M, Bald R, Hansmann M. First-trimester diagnosis of fetal congenital heart disease by transvaginal two-dimensional and Doppler echocardiography. Obstet Gynecol. 1990. 75:496–498.16. Bronshtein M, Zimmer EZ, Milo S, Ho SY, Lorber A, Gerlis LM. Fetal cardiac abnormalities detected by transvaginal sonography at 12-16 weeks’ gestation. Obstet Gynecol. 1991. 78:374–378.17. Gembruch U, Knopfle G, Bald R, Hansmann M. Early diagnosis of fetal congenital heart disease by transvaginal echocardiography. Ultrasound Obstet Gynecol. 1993. 3:310–317.18. Carvalho JS, Moscoso G, Tekay A, Campbell S, Thilaganathan B, Shinebourne EA. Clinical impact of first and early second trimester fetal echocardiography on high risk pregnancies. Heart. 2004. 90:921–926.19. Hyett JA, Perdu M, Sharland GK, Snijders RS, Nicolaides KH. Increased nuchal translucency at 10-14 weeks of gestation as a marker for major cardiac defects. Ultrasound Obstet Gynecol. 1997. 10:242–246.20. Matias A, Huggon I, Areias JC, Montenegro N, Nicolaides KH. Cardiac defects in chromosomally normal fetuses with abnormal ductus venosus blood flow at 10-14 weeks. Ultrasound Obstet Gynecol. 1999. 14:307–310.21. Tei C, Ling LH, Hodge DO, Bailey KR, Oh JK, Rodeheffer RJ, et al. New index of combined systolic and diastolic myocardial performance: a simple and reproducible measure of cardiac function-a study in normals and dilated cardiomyopathy. J Cardiol. 1995. 26:357–366.22. Hernandez-Andrade E, Lopez-Tenorio J, Figueroa-Diesel H, Sanin-Blair J, Carreras E, Cabero L, et al. A modified myocardial performance (Tei) index based on the use of valve clicks improves reproducibility of fetal left cardiac function assessment. Ultrasound Obstet Gynecol. 2005. 26:227–232.23. Api O, Emeksiz MB, Api M, Ugurel V, Unal O. Modified myocardial performance index for evaluation of fetal cardiac function in pre-eclampsia. Ultrasound Obstet Gynecol. 2009. 33:51–57.24. Hernandez-Andrade E, Crispi F, Benavides-Serralde JA, Plasencia W, Diesel HF, Eixarch E, et al. Contribution of the myocardial performance index and aortic isthmus blood flow index to predicting mortality in preterm growth-restricted fetuses. Ultrasound Obstet Gynecol. 2009. 34:430–436.25. Figueroa H, Silva MC, Kottmann C, Viguera S, Valenzuela I, Hernandez-Andrade E, et al. Fetal evaluation of the modified-myocardial performance index in pregnancies complicated by diabetes. Prenat Diagn. 2012. 32:943–948.26. Van Mieghem T, Klaritsch P, Done E, Gucciardo L, Lewi P, Verhaeghe J, et al. Assessment of fetal cardiac function before and after therapy for twin-to-twin transfusion syndrome. Am J Obstet Gynecol. 2009. 200:400.e1–400.e7.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Fetal Atrial Flutter Treated by Antiarrhythmic Agent to the Mother
- Transplacental Fetal Therapy for a Case of Fetal Supraventricular Tachycardia which Caused Fetal Hydrops
- How to perform a functional assessment of the fetal heart: a pictorial review
- A Case of Fetal Intracardiac Tumor Detected on Fetal Echocardiography
- Estimating Fetal Cardiac Output by Doppler Echocardiography
