Korean J Health Promot.
2014 Mar;14(1):33-42. 10.15384/kjhp.2014.14.1.33.
Effects of Multi-Component Exercise and Retraining after Detraining on Functional Fitness and Cognitive Function in Elder People with Mild Dementia
- Affiliations
-
- 1Division of Silver Industry, Kangnam University, Yongin, Korea. yoni91@hotmail.com
- KMID: 2305049
- DOI: http://doi.org/10.15384/kjhp.2014.14.1.33
Abstract
- BACKGROUND
With rapid growth in the number of older Koreans and prevalence of dementia, exercise has been emphasized as first, second and third prevention of dementia. A few study, however, investigate effects of detraining and retraining in demented elders. Therefore, the purpose of this study was to investigate the effects of 24 week exercise followed by 12 week detraining and retraining on physical and cognitive function in demented seniors.
METHODS
Thirty-five demented older adults were assigned into exercise and control group. Exercise group performed multi-component exercise, 2 times a week for 24 weeks. After 12 week detraining, subjects were retraining for 12 weeks. Subjects were tested four times on physiological variables, physical function and cognitive function. Ten subjects in exercise group and 6 subjects in control group were remained at final 48 week, and data from them were analyzed.
RESULTS
There were no significant effects on physiological variable in both groups. However, 24 week exercise improved upper and lower body strength, flexibility, dynamic mobility and physical function. These effects, however, were significantly decreased in 12 week detraining period and increased again after 12 week retraining. There were significance group differences. Cognitive function was improved after 24 week exercise but decreased in detraining and retraining period and no significant difference between groups was shown.
CONCLUSIONS
The present study suggests that positive effects after exercise tend to be reduced once one stops exercise, and be improved again after retraining. Therefore, strategies to encourage demented elders to exercise are needed.
MeSH Terms
Figure
-
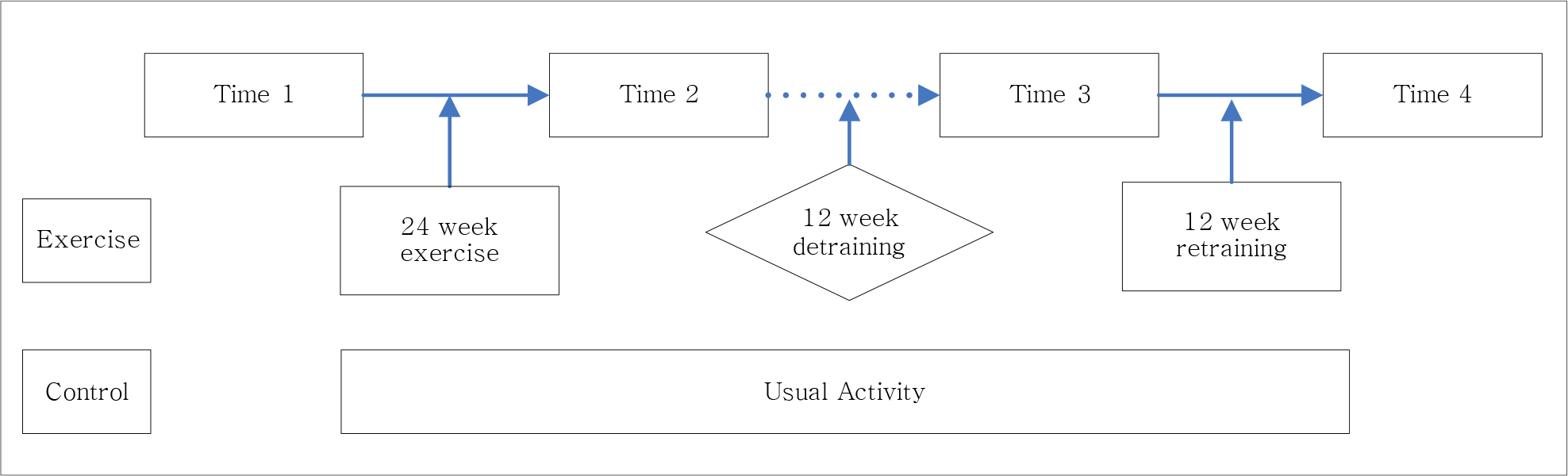
Fig. 1. Time 1, time 2, time 3, and time 4 indicate baseline, after 24 week exercise, after 12 week detraining, and after 12 week retraining respectively.
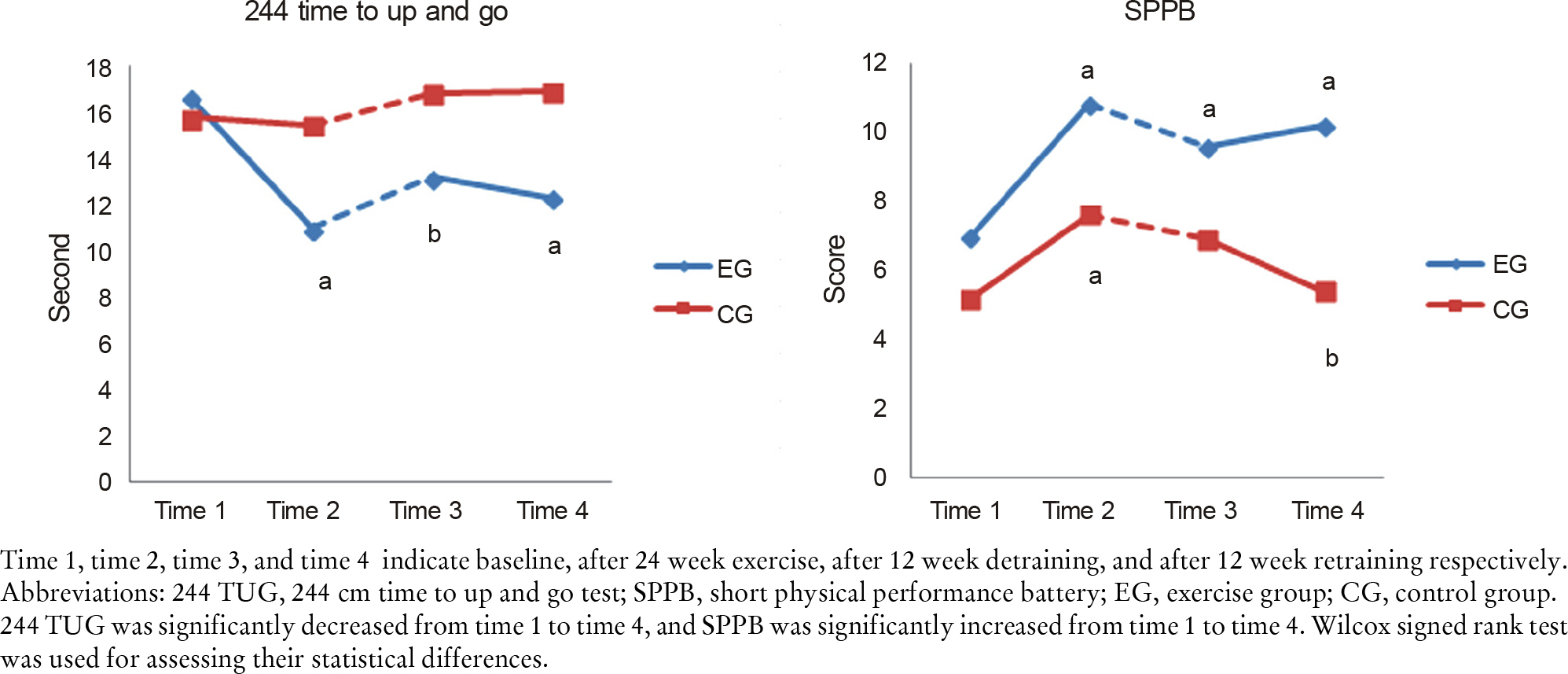
Fig. 2. Time 1, time 2, time 3, and time 4 indicate baseline, after 24 week exercise, after 12 week detraining, and after 12 week retraining respectively. Abbreviations: 244 TUG, 244 cm time to up and go test; SPPB, short physical performance battery; EG, exercise group; CG, control group. 244 TUG was significantly decreased from time 1 to time 4, and SPPB was significantly increased from time 1 to time 4. Wilcox signed rank test was used for assessing their statistical differences.
Reference
-
References
1. National Health Insurance Services. Fight with dementia. 2013.2. Costa PT, WIlliams TF, Somerfield M. Recognition and initial assessment of Alzheimer's diease and related dementias. Clinical practice guidelines no 19. Rockville: US Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research;1996.3. Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults. Psychological Science. 2003; 14(2):125–30.
Article4. Munoz VM, van Kan GA, Cantet C, Cortes F, Ousset PJ, Rolland Y, et al. Gait and balance impairments in Alzheimer disease patients. Alzheimer Dis Assoc Disord. 2010; 24(1):79–84.5. Rolland Y, Pillard F, Klapouszczak A, Reynish E, Thomas D, Andrieu S, et al. Exercise program for nursing home residents with Alzheimer's disease: a 1-year randomized, controlled trial. J Am Geriatr Soc. 2007; 55(2):158–65.
Article6. Kwak YS, Um SY, Son TG, Kim DJ. Effect of regular exercise on senile dementia patients. Int J Sports Med. 2008; 29(6):471–4.
Article7. Williams CL, Tappen RM. Exercise training for depressed older adults with Alzheimer's disease. Aging and Mental Health. 2008; 12(1):72–80.
Article8. Dishman RK. Exercise adherence: its impact on public health. Human Kinetics;1988.9. Cohen J. Statistical power analysis for the behavioral sciences. Psychology Press;1988.10. Heyn P, Abreu BC, Ottenbacher KJ. The effects of exercise training on elderly persons with cognitive impairment and dementia: a metaanalysis. Arch Phys Med Rehabil. 2004; 85(10):1694–704.11. Rikli RE, Jones CJ. Senior fitness test manual. Champaign, Ill; Leeds: Human Kinetics;2001. xiv,. p. 161. p.12. Cho BL. Physical performance measures in the elderly. Korean J Fam Med. 2003; 24(8):689–95. http://www.komci.org/CedRef. Full.php?ArticleID=1001KJFM%2F2003.24.8.689.13. Hong S. An investigation of the validity of thirty-second chair stand test as a measure of lower body strength in Korean older adults. International Journal of Human Movement Science. 2012; 6(1):17–28.14. Van Pelt RE, Evans EM, Schechtman KB, Ehsani AA, Kohrt WM. Contribution of total and regional fat mass to risk for cardiovascular disease in older women. American Journal of Physiology, Endocrinology and Metabolism. 2002; 282:E1023–8.15. Whitmer RA, Gustafson DR, Barrett-Connor E, Haan MN, Gunderson EP, Yaffe K. Central obesity and increased risk of dementia more than three decades later. Neurology. 2008; 71(14):1057–64.
Article16. Fratiglioni L, Launer LJ, Andersen K, Breteler MM, Copeland JR, Dartigues JF, et al. Incidence of dementia and major subtypes in Europe: a collaborative study of population-based cohorts. Neurologic Diseases in the Elderly Research Group. Neurology. 2000; 54(11 Suppl 5):S10–5.17. Andersen CK, Wittrup-Jensen KU, Lolk A, Andersen K, Kragh-S⊘rensen P. Ability to perform activities of daily living is the main factor affecting quality of life in patients with dementia. Health and Quality of Life Outcomes. 2004; 2(1):52–8.18. Bullock R, Hammond G. Realistic expectations: the management of severe Alzheimer disease. Alzheimer Dis Assoc Disord. 2003; 17:S80–5.
Article19. Kovach CR, Henschel H. Planning activities for patients with dementia: a descriptive study of therapeutic activities on special care units. J Gerontol Nurs. 1996; 22(9):33–8.
Article20. Lee S, Lee J. The study on health-related physical fitness and bone mineral density in the elderly dementia and mild cognitive impairment. Korean Journal of Sports Sccience. 2011; 20(4):789–98.21. Dvorak RV, Poehlman ET. Appendicular skeletal muscle mass, physical activity, and cognitive status in patients with Alzheimer's disease. Neurology. 1998; 51(5):1386–90.
Article22. Um S, Kwak Y. The effects of regular exercise on cognitive function and blood Lipid in woman patient with senile dementia. Korean Journal of Sports Science. 2004; 15(1):57–65. http://www.papersearch.net/view/detail.asp?detail_key=1m200283.23. Brill PA, Drimmer AM, Morgan LA, Gordon NF. The feasibility of conducting strength and flexibility programs for elderly nursing home residents with dementia. Gerontologist. 1995; 35(2):263–6.24. Winters KM, Snow CM. Detraining reverses positive effects of exercise on the musculoskeletal system in premenopausal women. J Bone Miner Res. 2000; 15(12):2495–503.
Article25. Son H. The Effects of exercise program on activities of daily living and balance in elderly with dementia. [dissertation]. Daegu: Daegu University;2007.26. Park H. The effects of in-facility exercise program on fall-related fitness and cognitive function in elderly with dementia. J Korean Soc Living Environ Sys. 2010; 17(1):77–85.27. van Gelder BM, Tijhuis MAR, Kalmijn S, Giampaoli S, Nissinen A, Kromhout D. Physical activity in relation to cognitive decline in elderly men. Neurology. 2004; 63(12):2316–21.
Article28. Lautenschlager NT, Cox KL, Flicker L, Foster JK, van Bockxmeer FM, Xiao J, et al. Effect of physical activity on cognitive function in older adults at risk for Alzheimer disease. JAMA. 2008; 300(9):1027–37.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Therapeutic Exercise Strategies in Patients with Dementia
- The Effect of Multi-tasking Exercise Intervention on Cognitive Function in Elderly and Cognitive Impairment Patients: a Pilot Multicenter Study
- Effect of a Physical-Strengthening Exercise Program on Physical Fitness, Depression, and Cognitive Function in Older Patients with Parkinson's Disease: A Cross-Sectional Study
- The Clinical Significance of Cognitive Interventions for the Patients with Mild Cognitive Impairment
- Effects of Cognitive-based Interventions of Older Adults with Mild Cognitive Impairment: A Systematic Review and Meta-analysis
