The Use of a Corrective Procedure with Vicryl Mesh for Oncoplastic Surgery of the Breast
- Affiliations
-
- 1Division of Breast and Endocrine Surgery, College of Medicine, Hallym University, Anyang, Korea. lskim0503@hallym.ac.kr
- KMID: 2286577
- DOI: http://doi.org/10.4048/jbc.2009.12.1.36
Abstract
-
PURPOSE: In addition to the oncological results, cosmetic results are very important to cancer patients. Currently, the use of oncoplastic surgery is an emerging approach. In this study, we examined the clinical outcomes of the use of a corrective procedure with an absorbable implant, a Vicryl mesh(R), as compared with the use of conventional breast conserving surgery (BCS).
METHODS
Fifty six patients who completed questionnaire were enrolled in the study. For 33 cases, BCS was performed concurrently with the use of a Vicryl mesh and for the other 23 cases, conventional BCS alone was performed. Contraindications of the use of corrective procedure were a patient age over 60 year, diabetes, neoadjuvant chemotherapy and a previous excisional biopsy performed on the same breast. Patients rated their cosmetic outcomes by use of a four point scale.
RESULTS
For one of 34 cases, the Vicryl mesh was removed due to infection and this patient was excluded from the study. Twenty seven of the remaining 33 patients (82%) who underwent the corrective procedure with Vicryl mesh were satisfied with their outcome. For patients that received conventional BCS only ten of 23 patients (43%) were satisfied with their outcome (p=0.05). Patient age, body mass index (BMI) and tumor location did not affect the cosmetic outcomes of the corrective procedure. When the resection area of the breast was 40-70 cm2, 88% of the patients were satisfied with their outcome.
CONCLUSION
This study suggested that the use of Vicryl mesh correction was superior to the use of conventional BCS alone for cosmesis. This method appears to provide a satisfactory outcome for oncoplastic surgery of the breast.
Keyword
MeSH Terms
Figure
-
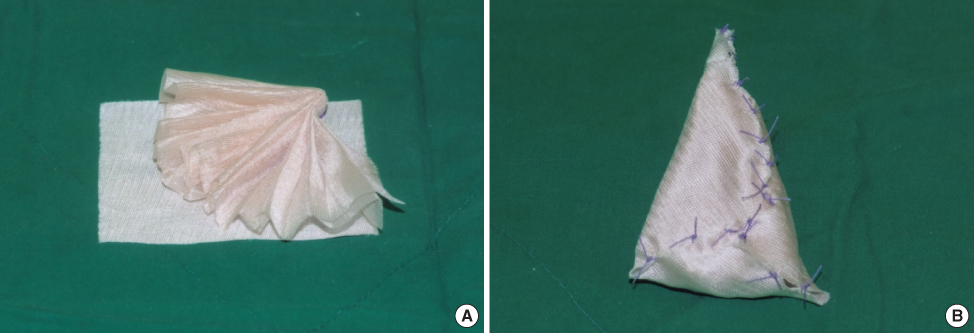
Figure 1 The method of making absorbable implant. (A) Vcryl mesh wrapped with Interceed® (7.6×10.2 cm). (B) Completion of absorbable implant.

Figure 2 The application of the absorbable implant. This absorbable implant was put into the dead space. And we fixed this material to the breast parenchyme with vicryl suture. To prevent surgical site infection, subcutaneous layer was closed very tightly.
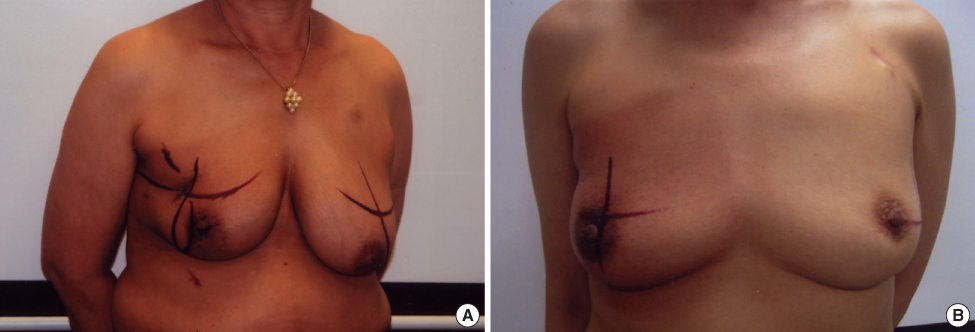
Figure 3 The comparison between Vicryl mesh correction group with conventional BCS during radiation therapy. (A) Frontal view of the patient with conventional BCS. (B) Frontal view of the patient with Vicryl mesh. These patients received radiation therapy 6 months after surgery. There was no additional changes of breast contour during radiation therapy and no radiation skin ulcer at the vicryl mesh graft area.
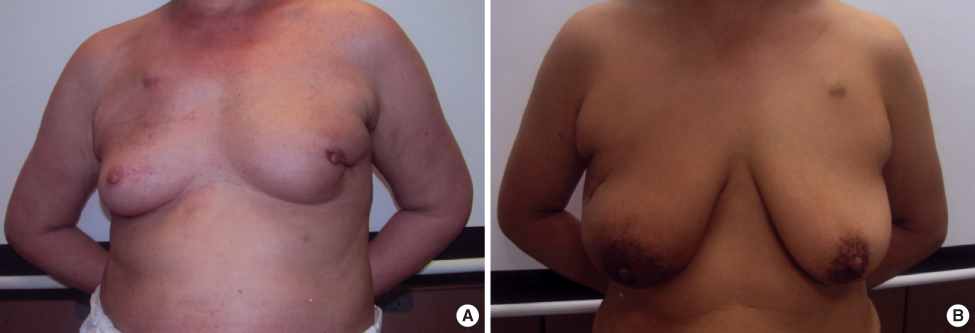
Figure 4 Postoperative figures one year after surgery. (A) Frontal view of the patient with conventional BCS. (B) Frontal view of the patient with Vicryl mesh correction. All of these patients had been treated with adjuvant chemotherapy and radiation therapy. There was little displacement of nipple and areola in vicryl mesh correction case. And also, there was no significant skin dimpling in vicryl mesh correction case.
Cited by 4 articles
-
Results from Over One Year of Follow-Up for Absorbable Mesh Insertion in Partial Mastectomy
Min Young Koo, Se Kyung Lee, Sung Mo Hur, Soo Youn Bae, Min-Young Choi, Dong Hui Cho, Sangmin Kim, Jun-Ho Choe, Jung-Han Kim, Jee Soo Kim, Jeong Eon Lee, Seok Jin Nam, Jung-Hyun Yang
Yonsei Med J. 2011;52(5):803-808. doi: 10.3349/ymj.2011.52.5.803.Nationwide Survey of the Use of Absorbable Mesh in Breast Surgery in Korea
Ku Sang Kim, Man Young Park, Woo Jae Kim, Kuk Young Na, Yong Sik Jung, Young Jin Choi, Yong Lai Park, Se-Jeong Oh, Hyuk-Jae Shin,
J Breast Cancer. 2009;12(3):210-214. doi: 10.4048/jbc.2009.12.3.210.Analysis of Infections Occurring in Breast Cancer Patients after Breast Conserving Surgery Using Mesh
Jin Seong Cho, Sun Hyoung Shin, Ji Young Park, Young Ju Song, Jeong Min Yi, Min Ho Park, Jung Han Yoon, Young Jong Jegal, Ji Sin Yi, Seong Ja An, Hwo Soon Lim
J Breast Cancer. 2011;14(4):328-332. doi: 10.4048/jbc.2011.14.4.328.The Suitability of Absorbable Mesh Insertion for Oncoplastic Breast Surgery in Patients with Breast Cancer Scheduled to Be Irradiated
Taehyun Kim, Heunglae Cho
J Breast Cancer. 2013;16(1):84-89. doi: 10.4048/jbc.2013.16.1.84.
Reference
-
1. Vallejo da Silva A, Destro C, Torres W. Oncoplastic surgery of the breast: rationale and experience of 30 cases. Breast. 2007. 16:411–419.
Article2. Wang HT, Barone CM, Steigelman MB, Kahlenberg M, Rousseau D, Berger J, et al. Aesthetic outcomes in breast conservation therapy. Aeshetic Surg J. 2008. 28:165–170.
Article3. Cho HJ, Kwak KH, Kim JR, Sohn SC, Park KM, Han SH. Feasibility of concurrent adjuvant chemotherapy and rdiotherapy after breast-conserving surgery in early breast cancer. J Korean Breast Cancer Soc. 2004. 4:289–293.4. Fisher B, Bauer M, Margolese R, Poisson R, Redmond C, Fisher E. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985. 312:665–673.
Article5. Clough KB, Lewis JS, Fitoussi A, Faucoult MC. Oncoplastic techniques allow extensive resection for breast-conserving therapy of breast carcinomas. Ann Surg. 2003. 237:26–34.
Article6. Rietjens M, Urban CA, Rey PC, Mazzarol G, Maisonneuve P, Garusi C, et al. Long-term oncological results of breast conservative treatment with oncoplastic surgery. Breast. 2007. 16:387–395.
Article7. Gianetta E, Cian F, Cuneo S, Friedman D, Vitale B, Marinari G, et al. Hernia repair in elderly patients. Br J Surg. 1997. 84:983–985.
Article8. Sanuki J, Fukuma E, Wadamori K, Higa K, Sakamoto N, Tsunda Y. Volume replacement with polyglycolic acid mesh for correcting breast deformity after endoscopic conservative surgery. Clin Breast Cancer. 2005. 6:175.
Article9. Góes JC, Landecker A, Lyra EC, Henríquez LJ, Góes RS, Godoy PM. The application of mesh support in periareolar breast surgery: clinical and mammographic evaluation. Aesthetic Plat Surg. 2004. 28:268–274.
Article10. Góes JC. Periareolar mammaplasty: double skin technique with application of polyglactine or mixed mesh. Plast Reconstr Surg. 1996. 97:959–968.
Article11. Petit J, Rietjens M, Garusi C. Breast reconstructive techniques in cancer patients: which ones, when to apply, which immediate and long term risks? Crit Rev Oncol Hematol. 2001. 38:231–239.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical Repair of the Kidney after Blunt Renal Injury Using a Vicryl Mesh an Experimental Study
- Oncoplastic Breast Surgery
- Volume Replacement with Polyglactin 910 Mesh for Breast Reconstruction after Endoscopy-Assisted Breast Conserving Surgery for Treating Early Breast Cancer: the Early Results
- Comparison between the Exposure Rates of Tutoplast(R) and Vicryl Mesh Used as Wrapping Materials for Hydroxyapatite Orbital Implant
- The Use of Absorbable Surgical Mesh after Partial Mastectomy for Improving the Cosmetic Outcome
