The Differences of Left Ventricular Geometry in Acute Myocardial Infarction and the Effects on Short Term Mortality
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Ewha Womans University School of Medicine, Seoul, Korea. giljshin@ewha.ac.kr
- KMID: 2284012
- DOI: http://doi.org/10.12771/emj.2013.36.1.26
Abstract
OBJECTIVES
This study designed to find the differences of left ventricular (LV) geometry in acute myocardial infarction (AMI) between ST elevation myocardial infarction (STEMI) and non ST elevation myocardial infarction (NSTEMI) and the occurrences of adverse outcome according to the LV geometry.
METHODS
Comprehensive echocardiographic analyses were performed in 256 patients with AMI. The left ventricular mass index (LVMI) and relative wall thickness (RWT) were calculated. LV geometry were classified into 4 groups based on RWT and LVMI: normal geometry (normal LVMI and normal RWT), concentric remodeling (normal LVMI and increased RWT), eccentric hypertrophy (increased LVMI and normal RWT), and concentric hypertrophy (increased LVMI and increased RWT). Cox proportional hazards models were used to evaluate the relationships among LV geometry and clinical outcomes.
RESULTS
Patients with NSTEMI were more likely to have diabetes mellitus, hypertension, heart failure, stroke and previous myocardial infarction. By the geometric type, patients with NSTEMI were more likely to have eccentric hypertrophy (n=51, 34.7% vs. n=24, 22.0%, P=0.028). There was no significantly different adverse outcome between STEMI and NSTEMI patients. Fifteen patients (5.9%, 7 female [46.7%]) died and the median duration of survival was 10 days (range, 1 to 386 days). Concentric hypertrophy carried the greatest risk of all cause mortality (hazard ratios, 5.83; 95% confidence interval, 1.04 to 32.7).
CONCLUSION
NSTEMI patients had more likely to have eccentric hypertrophy but adverse outcome after AMI was not different between STEMI and NSTEMI patients. Concentric hypertrophy had the greatest risk of short term mortality.
Keyword
MeSH Terms
Figure
-

Fig. 1 Unadjusted hazard ratios (95% confidence intervals) for all cause mortality. Cox proportional hazards models are used. CI, confidence interval; DM, diabetes mellitus; HTN, hypertension; HF, heart failure; CR, concentric remodeling; EH, ecoentric hypertrophy; CH, concentric hypertrophy; Ref, referent value.
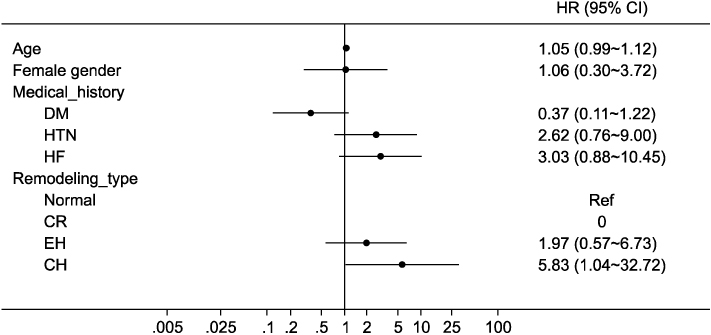
Fig. 2 Adjusted hazard ratios (95% confidence intervals) for all cause mortality. Multivariable Cox proportional hazards models are used. CI, confidence interval; DM, diabetes mellitus; HTN, hypertencsion; HF, heart failure; CR, concentric remodeling; EH, ecoentric hypertrophy; CH, concentric hypertrophy; Ref, referent value.

Fig. 3 Unadjusted hazard ratios (95% confidence intervals) for cardiovascular mortality. Cox proportional hazards models are used. CI, confidence interval; DM, diabetes mellitus; HTN, hypertension; HF, heart failure; CR, concentric remodeling; EH, ecoentric hypertrophy; CH, concentric hypertrophy; Ref, referent value.
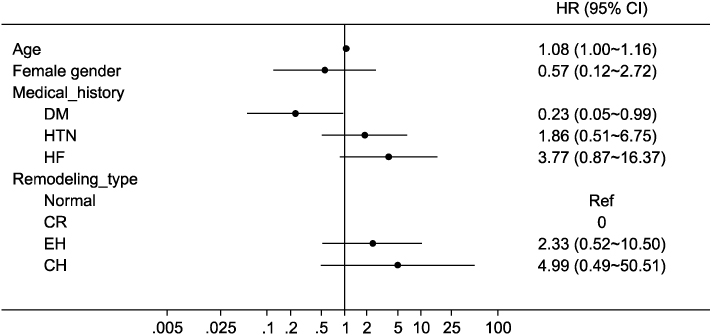
Fig. 4 Adjusted hazard ratios (95% confidence intervals) for cardiovascular mortality. Multivariable Cox proportional hazards models are used. CI, confidence interval; DM, diabetes mellitus; HTN, hypertencsion; HF, heart failure; CR, concentric remodeling; EH, ecoentric hypertrophy; CH, concentric hypertrophy; Ref, referent value.
Reference
-
1. Hunt SA. American College of Cardiology. American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol. 2005. 46:e1–e82.2. Kim SS, Jeon HK, Cho GM, Lee JH, Kim SJ, Park MY, et al. Evaluation of cardiac function by transthoracic echocardiography in subjects with st-segment elevation myocardial infarction following primary percutaneous coronary intervention according to valsartan dose: the valsartan one center trial. J Cardiovasc Ultrasound. 2010. 18:77–83.3. Gaasch WH, Zile MR. Left ventricular structural remodeling in health and disease: with special emphasis on volume, mass, and geometry. J Am Coll Cardiol. 2011. 58:1733–1740.4. Gaasch WH. Left ventricular radius to wall thickness ratio. Am J Cardiol. 1979. 43:1189–1194.5. Castello Brescane R. The prognostic significance of left ventricular geometry: fantasy or reality? Rev Esp Cardiol. 2009. 62:235–238.6. Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Relation of left ventricular mass and geometry to morbidity and mortality in uncomplicated essential hypertension. Ann Intern Med. 1991. 114:345–352.7. Verma A, Meris A, Skali H, Ghali JK, Arnold JM, Bourgoun M, et al. Prognostic implications of left ventricular mass and geometry following myocardial infarction: the VALIANT (VALsartan In Acute myocardial iNfarcTion) Echocardiographic Study. JACC Cardiovasc Imaging. 2008. 1:582–591.8. Carluccio E, Tommasi S, Bentivoglio M, Buccolieri M, Filippucci L, Prosciutti L, et al. Prognostic value of left ventricular hypertrophy and geometry in patients with a first, uncomplicated myocardial infarction. Int J Cardiol. 2000. 74:177–183.9. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography's Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005. 18:1440–1463.10. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I, et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol. 1986. 57:450–458.11. Sutton MG, Sharpe N. Left ventricular remodeling after myocardial infarction: pathophysiology and therapy. Circulation. 2000. 101:2981–2988.12. Pfeffer MA, Braunwald E. Ventricular remodeling after myocardial infarction. Experimental observations and clinical implications. Circulation. 1990. 81:1161–1172.13. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990. 322:1561–1566.14. Ghali JK, Kadakia S, Cooper RS, Liao YL. Impact of left ventricular hypertrophy on ventricular arrhythmias in the absence of coronary artery disease. J Am Coll Cardiol. 1991. 17:1277–1282.15. Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Left ventricular mass and incidence of coronary heart disease in an elderly cohort. The Framingham Heart Study. Ann Intern Med. 1989. 110:101–107.16. Vakili BA, Okin PM, Devereux RB. Prognostic implications of left ventricular hypertrophy. Am Heart J. 2001. 141:334–341.17. Chahal NS, Lim TK, Jain P, Chambers JC, Kooner JS, Senior R. New insights into the relationship of left ventricular geometry and left ventricular mass with cardiac function: A population study of hypertensive subjects. Eur Heart J. 2010. 31:588–594.18. Hwang JW, Kang SJ, Lim HS, Choi BJ, Choi SY, Hwang GS, et al. Impact of arterial stiffness on regional myocardial function assessed by speckle tracking echocardiography in patients with hypertension. J Cardiovasc Ultrasound. 2012. 20:90–96.19. Erlebacher JA, Weiss JL, Eaton LW, Kallman C, Weisfeldt ML, Bulkley BH. Late effects of acute infarct dilation on heart size: a two dimensional echocardiographic study. Am J Cardiol. 1982. 49:1120–1126.20. Pfeffer MA, Pfeffer JM. Ventricular enlargement and reduced survival after myocardial infarction. Circulation. 1987. 75(5 Pt 2):IV93–IV97.21. St John Sutton M, Pfeffer MA, Plappert T, Rouleau JL, Moye LA, Dagenais GR, et al. Quantitative two-dimensional echocardiographic measurements are major predictors of adverse cardiovascular events after acute myocardial infarction: the protective effects of captopril. Circulation. 1994. 89:68–75.22. White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, Wild CJ. Left ventricular end-systolic volume as the major determinant of survival after recovery from myocardial infarction. Circulation. 1987. 76:44–51.23. Konstam MA, Udelson JE, Anand IS, Cohn JN. Ventricular remodeling in heart failure: a credible surrogate endpoint. J Card Fail. 2003. 9:350–353.24. Konstam MA. Patterns of ventricular remodeling after myocardial infarction: clues toward linkage between mechanism and morbidity. JACC Cardiovasc Imaging. 2008. 1:592–594.25. Ghali JK, Liao Y, Cooper RS. Influence of left ventricular geometric patterns on prognosis in patients with or without coronary artery disease. J Am Coll Cardiol. 1998. 31:1635–1640.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Incidence of Left Ventricular Thrombus after Acute Myocardial Infarction
- Two Cases of Successful Surgical Treatment of Postmyocardial Infarction Ventricular Septal Defect-Repeated Performation After the First Operation
- Three Cases of Ventricular Septal Rupture after Acute Myocardial Infarction
- Assessment of Left and Right Ventricular Performance by Gated Blood Pool Scan in Acute Transmural Myocardial Infarction
- Two-Dimensional Echocardiographic Predictors of Ventricular Enlargement after Acute Myocardial Infarction
