Treatment Failure after Uterine Artery Embolization for Symptomatic Uterine Fibroids: Significance of Ovarian Arterial Collateral Vessels in Predicting the Outcome
- Affiliations
-
- 1Department of Radiology, Ewha Womans University School of Medicine, Seoul, Korea. kangbc@ewha.ac.kr
- KMID: 2284000
- DOI: http://doi.org/10.12771/emj.2012.35.2.102
Abstract
OBJECTIVES
To evaluate the treatment failure (TF) rate of leiomyoma after uterine artery embolization (UAE) for uterine leiomyomas in cases of the presence of anastomoses between the ovarian arteries (OA) and uterine arteries (UA).
METHODS
The results of 163 consecutive UAE for uterine fibroid were reviewed. Mean patient age was 42.8 years (range, 25 to 57 years). TF was evaluated according to the anastomoses between OA and UA on pre-embolization angiography. Magnetic resonance images (MRIs) were obtained at 1~6 months or 12 months after UAE. MRIs were gadolinium (Gd)-enhanced images and/or T2-weighted images. MRIs exhibited focal enhancement portion on fibroid and evaluated the TF rate of the leiomyoma in patients of presence of anastomoses between OA and UA.
RESULTS
Fifty six patients had anastomoses between UA and OA on pre-embolization angiography (56/163, 34.4%). Angiographic subtypes were type Ia (n=19), type Ib (n=16), type II (n=11) and type III (n=10). Of all patients, 10 patients showed the focal enhancements of the leiomyomas on follow-up enhanced MRIs (10/163, 6.1%). Three treatments failed in patients demonstrated type Ia (3/19, 15,8%). One had type Ib (1/16, 6.3%). Other 6 had no anastomoses. There was no TF rate difference between patients with communication (4/56, 7.1%) and without communication (6/107, 5.7%). However, TF rate in patients with type Ia communication (15.8%) was higher than that without communication (5.7%; P<0.05).
CONCLUSION
Type Ia utero-ovarian anastomoses communication could be a contraindication for embolization treatment for leiomyoma.
MeSH Terms
Figure
-
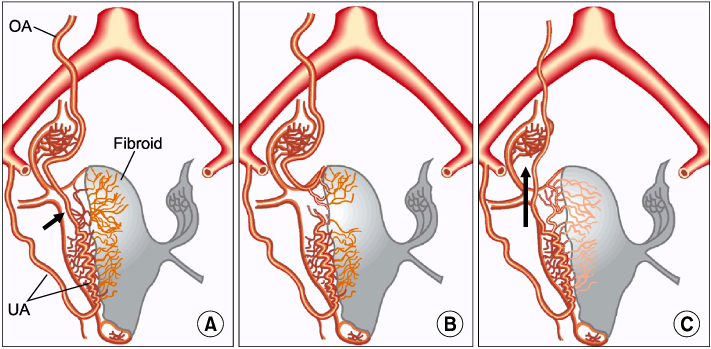
Fig. 1 Types of ovarian artery to uterine artery anastomoses. (A) Type I ovarian artery to uterine artery anastomoses. The ovarian artery connects to the intramural uterine artery before the fibroid supply through the tubo-ovarian segment (arrow). (B) Type II ovarian artery to uterine artery anastomosis. The ovarian artery supplies the fibroid directly, without prior connection to the uterine artery. (C) Type III ovarian artery to uterine artery anastomosis. The ovarian supply is at least in part from the uterine artery, with flow in the tubo-ovarian segment toward the ovary. Arrow indicates the direction of flow. OA, ovarian artery; UA, uterine artery.
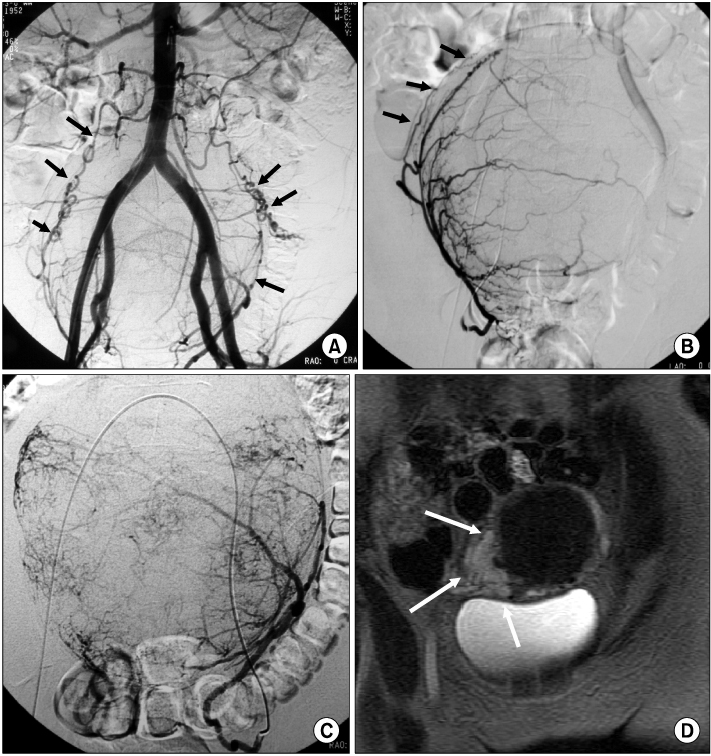
Fig. 2 Bilateral type Ia anastomoses in a 46-year-old woman with treatment failure. (A) Pre-embolization anteroposterior abdominal aortogram shows opacification of the both ovarian arteries (arrows). (B, C) Selective right uterine angiograms in anteroposterior projection show typical myomatous blush without evidence of contrast material reflux into the tubo-ovarian segment (arrows). (D) MR image 4 months after uterine artery embolization shows focal peripheral enhancements (white arrows).
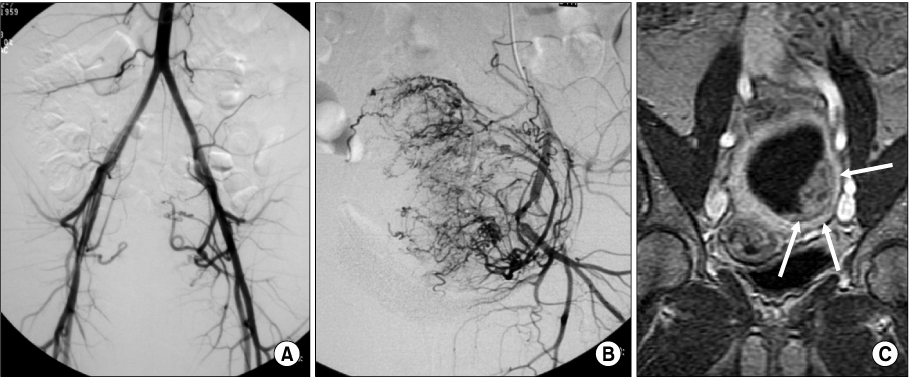
Fig. 3 Treatment failure in a 35-year-old woman without anastomosis between ovarian artery-to-uterine artery. (A) Pre-embolization anteroposterior abdominal aortogram and (B) left uterine selective uterine angiogram shows myomatous blushes without opacification of contrast material without evidence into the tubo-ovarian segment. (C) MR image 2 months after uterine artery embolization shows focal peripheral enhancement (white arrows).
Reference
-
1. Marshall LM, Spiegelman D, Barbieri RL, Goldman MB, Manson JE, Colditz GA, et al. Variation in the incidence of uterine leiomyoma among premenopausal women by age and race. Obstet Gynecol. 1997. 90:967–973.2. Goodwin SC, McLucas B, Lee M, Chen G, Perrella R, Vedantham S, et al. Uterine artery embolization for the treatment of uterine leiomyomata midterm results. J Vasc Interv Radiol. 1999. 10:1159–1165.3. Hutchins FL Jr, Worthington-Kirsch R. Embolotherapy for myoma-induced menorrhagia. Obstet Gynecol Clin North Am. 2000. 27:397–405.4. Spies JB, Scialli AR, Jha RC, Imaoka I, Ascher SM, Fraga VM, et al. Initial results from uterine fibroid embolization for symptomatic leiomyomata. J Vasc Interv Radiol. 1999. 10:1149–1157.5. Worthington-Kirsch RL, Popky GL, Hutchins FL Jr. Uterine arterial embolization for the management of leiomyomas: quality-of-life assessment and clinical response. Radiology. 1998. 208:625–629.6. Pelage JP, Le Dref O, Soyer P, Kardache M, Dahan H, Abitbol M, et al. Fibroid-related menorrhagia: treatment with superselective embolization of the uterine arteries and midterm follow-up. Radiology. 2000. 215:428–431.7. Hutchins FL Jr, Worthington-Kirsch R, Berkowitz RP. Selective uterine artery embolization as primary treatment for symptomatic leiomyomata uteri. J Am Assoc Gynecol Laparosc. 1999. 6:279–284.8. Nikolic B, Spies JB, Abbara S, Goodwin SC. Ovarian artery supply of uterine fibroids as a cause of treatment failure after uterine artery embolization: a case report. J Vasc Interv Radiol. 1999. 10:1167–1170.9. Pelage JP, Jacob D, Le Dref O, Laurent A. Re: Leiomyoma recurrence after uterine artery embolization. J Vasc Interv Radiol. 2004. 15:773.10. Spies JB. Uterine artery embolization for fibroids: understanding the technical causes of failure. J Vasc Interv Radiol. 2003. 14:11–14.11. Matson M, Nicholson A, Belli AM. Anastomoses of the ovarian and uterine arteries: a potential pitfall and cause of failure of uterine embolization. Cardiovasc Intervent Radiol. 2000. 23:393–396.12. Razavi MK, Wolanske KA, Hwang GL, Sze DY, Kee ST, Dake MD. Angiographic classification of ovarian artery-to-uterine artery anastomoses: initial observations in uterine fibroid embolization. Radiology. 2002. 224:707–712.13. Burn PR, McCall JM, Chinn RJ, Vashisht A, Smith JR, Healy JC. Uterine fibroleiomyoma: MR imaging appearances before and after embolization of uterine arteries. Radiology. 2000. 214:729–734.14. deSouza NM, Williams AD. Uterine arterial embolization for leiomyomas: perfusion and volume changes at MR imaging and relation to clinical outcome. Radiology. 2002. 222:367–374.15. Jha RC, Ascher SM, Imaoka I, Spies JB. Symptomatic fibroleiomyomata: MR imaging of the uterus before and after uterine arterial embolization. Radiology. 2000. 217:228–235.16. Chrisman HB, West D, Corpuz B, Ryu RK, Salem R, Carr J, et al. Primary failure of uterine artery embolization: use of magnetic resonance imaging to select patients for repeated embolization. J Vasc Interv Radiol. 2005. 16:1143–1147.17. Marret H, Cottier JP, Alonso AM, Giraudeau B, Body G, Herbreteau D. Predictive factors for fibroids recurrence after uterine artery embolisation. BJOG. 2005. 112:461–465.18. Goodwin SC, Vedantham S, McLucas B, Forno AE, Perrella R. Preliminary experience with uterine artery embolization for uterine fibroids. J Vasc Interv Radiol. 1997. 8:517–526.19. Marret H, Alonso AM, Cottier JP, Tranquart F, Herbreteau D, Body G. Leiomyoma recurrence after uterine artery embolization. J Vasc Interv Radiol. 2003. 14:1395–1399.20. Walker WJ, Pelage JP. Uterine artery embolisation for symptomatic fibroids: clinical results in 400 women with imaging follow up. BJOG. 2002. 109:1262–1272.21. McLucas B, Adler L, Perrella R. Uterine fibroid embolization: nonsurgical treatment for symptomatic fibroids. J Am Coll Surg. 2001. 192:95–105.22. Smith SJ, Sewall LE, Handelsman A. A clinical failure of uterine fibroid embolization due to adenomyosis. J Vasc Interv Radiol. 1999. 10:1171–1174.23. Jha RC, Takahama J, Imaoka I, Korangy SJ, Spies JB, Cooper C, et al. Adenomyosis: MRI of the uterus treated with uterine artery embolization. AJR Am J Roentgenol. 2003. 181:851–856.24. Kim MD, Won JW, Lee DY, Ahn CS. Uterine artery embolization for adenomyosis without fibroids. Clin Radiol. 2004. 59:520–526.25. Siskin GP, Tublin ME, Stainken BF, Dowling K, Dolen EG. Uterine artery embolization for the treatment of adenomyosis: clinical response and evaluation with MR imaging. AJR Am J Roentgenol. 2001. 177:297–302.26. Pelage JP, Guaou NG, Jha RC, Ascher SM, Spies JB. Uterine fibroid tumors: long-term MR imaging outcome after embolization. Radiology. 2004. 230:803–809.27. Marret H, Tranquart F, Sauget S, Alonso AM, Cottier JP, Herbreteau D. Contrast-enhanced sonography during uterine artery embolization for the treatment of leiomyomas. Ultrasound Obstet Gynecol. 2004. 23:77–79.28. Itkin M, Shlansky-Goldberg R. Uterine fibroid embolization for the treatment of symptomatic leiomyomata. Appl Radiol. 2002. 31(10):9–17.29. Worthington-Kirsch RL, Andrews RT, Siskin GP, Shlansky-Goldberg R, Lipman JC, Goodwin SC, et al. II. Uterine fibroid embolization: technical aspects. Tech Vasc Interv Radiol. 2002. 5:17–34.30. Sampson JA. The blood supply of uterine myomata. Surg Gynecol Obstet. 1912. 14:215–234.31. Lindenbaum E, Brandes JM, Itskovitz J. Ipsi- and contralateral anastomosis of the uterine arteries. Acta Anat (Basel). 1978. 102:157–161.32. Andrews RT, Bromley PJ, Pfister ME. Successful embolization of collaterals from the ovarian artery during uterine artery embolization for fibroids: a case report. J Vasc Interv Radiol. 2000. 11:607–610.33. Marx M, Wack JP, Baker EL, Stevens SK, Barakos JA. Ovarian protection by occlusion of uteroovarian collateral vessels before uterine fibroid embolization. J Vasc Interv Radiol. 2003. 14:1329–1332.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Uterine Fibroids Necrosis after Transarterial Embolization for Treatment of Uterine Fibroids
- A Case of Vaginal Expulsion of Submucosal Fibroid after Uterine Artery Embolization
- Aberrant Ovarian Artery Originating from the Iliolumbar Artery: A Case Report
- Uterine necrosis after partial obstruction of the uterine artery via selective embolization in postpartum hemorrhage: A case report
- Ovarian Protection by Selective Coil Embolization of a Uteroovarian Anastomosis before Uterine Fibroid Embolization: A Report of Two Cases
