Moderately Differentiated Neuroendocrine Carcinoma of the Larynx
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Korea University College of Medicine, Seoul, Korea. kyjung@kumc.or.kr
Abstract
- Neuroendocrine neoplasm of the larynx is a morphologically heterogeneous group of tumors. This unusual neoplasm includes the four different type of tumors. Paraganglioma is the best-known neural origin tumor. The epithelial origin tumor is further divided based on the degree of differentiation into well, moderately, and poorly differentiated carcinoma. The diverse biological behavior of neuroendocrine neoplasm of larynx makes an accurate diagnosis of paramount importance, since treatment depends on diagnostic accuracy. The diagnosis is based primarily on light microscopy, and immunohistochemical and/or ultrastructural investigations are needed to diagnose correctly. The mainstay of treatment of moderately differentiated neuroendocrine carcinoma of the larynx is surgery. Elective neck treatment should be performed considering the high likelihood of cervical lymph node metastases. The 5-yr survival rate approximates 50%, and 10-yr survival rate is only 30%.
Keyword
MeSH Terms
Figure
-
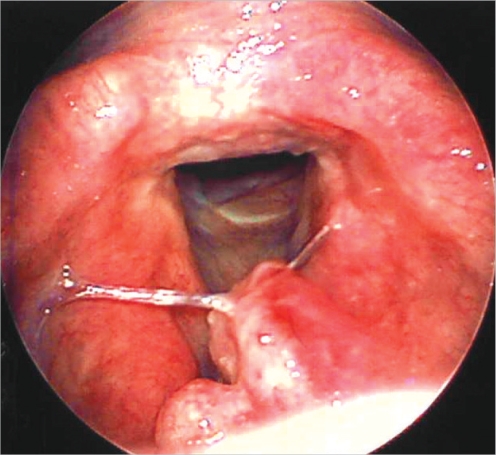
Fig. 1 Laryngoscopic image showing a submucosal mass involving laryngeal surface of the epiglottis. Both true vocal cords are mobile and the tumor has no glottic extension. Anterior commisure is free of tumor.
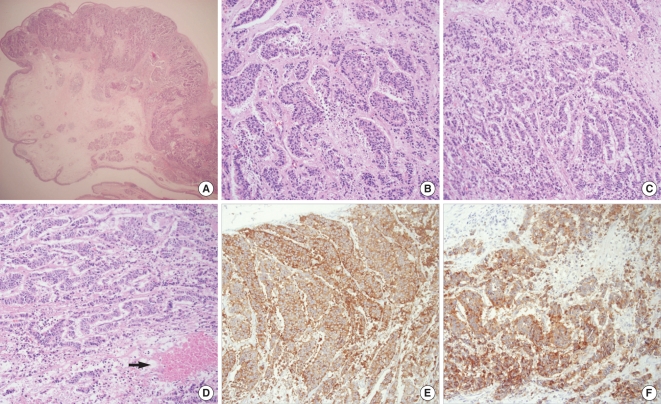
Fig. 2 Pathologic pictures. (A) Low power view with overlying intact mucosa (hematoxylin-eosin [H&E], magnification ×20). (B) High-power view showing pseudogland and rodget arrangement as a neuroendocrine differentiation (H&E, magnification ×200). (C) Cord and trabecular arrangement with nuclear and cellular pleomorphism (H&E, magnification ×200). (D) Tumor necrosis area (arrow) (H&E, magnification ×200). (E) Positive immunoreaction to chromogranin (magnification ×200). (F) Positive immunoreaction to synaptophysin (magnification ×200).

Fig. 3 The contrast-enhanced CT scans. (A) Supraglottic tumor invades the pre-epiglottic space. (B) Multiple neck metastases are seen at the left level II, III areas.

Fig. 4 At the follow-up of 6 months after operation. (A) Laryngoscopic image shows postradiation edema around previous operative area. But there is no evidence of local recurrence. (B) Bone scan image demonstrates multiple bone metastases (rib, spine, shoulder, skull base). (C) T1-weighted sagittal MRI scan shows metastatic lesions at T7, T11 level with compression fracture at L2 level (arrows). (D) Expansile metastatic lesion is noted at the right 7th rib (T1-weighted axial MRI scan, arrow).
Reference
-
1. Goldman NC, Hood CI, Singleton GT. Carcinoid of the larynx. Arch Otolaryngol. 1969; 7. 90(1):64–67. PMID: 5785991.
Article2. McBride LC, Righi PD, Krakovitz PR. Case study of well-differentiated carcinoid tumor of the larynx and review of laryngeal neuroendocrine tumors. Otolaryngol Head Neck Surg. 1999; 4. 120(4):536–539. PMID: 10187951.
Article3. Ferlito A, Barnes L, Rinaldo A, Gnepp DR, Milroy CM. A review of neuroendocrine neoplasms of the larynx: update on diagnosis and treatment. J Laryngol Otol. 1998; 9. 112(9):827–834. PMID: 9876371.
Article4. Hauser H, Wolf G, Uranus S, Klimpfinger M. Neuroendocrine tumors in various organ systems in a ten-year period. Eur J Surg Oncol. 1995; 6. 21(3):297–300. PMID: 7781801.5. Gillenwater A, Lewin J, Roberts D, El-Naggar A. Moderately differentiated neuroendocrine carcinoma (atypical carcinoid) of the larynx: a clinically aggressive tumor. Laryngoscope. 2005; 7. 115(7):1191–1195. PMID: 15995505.
Article6. Ferlito A, Rinaldo A. The spectrum of endocrinocarcinomas of the larynx. Oral Oncol. 2005; 10. 41(9):878–883. PMID: 16154516.
Article7. Chung JH, Lee SS, Shim YS, Kim SY, Nam SY, Kim DH, et al. A study of moderately differentiated neuroendocrine carcinomas of the larynx and an examination of non-neoplastic larynx tissue for neuroendocrine cells. Laryngoscope. 2004; 7. 114(7):1264–1270. PMID: 15235358.
Article8. Ferlito A, Shaha AR, Rinaldo A. Neuroendocrine neoplasms of the larynx: diagnosis, treatment and prognosis. ORL J Otorhinolaryngol Relat Spec. 2002; Mar–Apr. 64(2):108–113. PMID: 12021501.
Article
