Capacity of Rectified Vestibular Evoked Myogenic Potential in Correcting Asymmetric Muscle Contraction Power
- Affiliations
-
- 1Department of Otolaryngology-Head and Neck Surgery, Dankook University College of Medicine, Cheonan, Korea.
- 2Department of Otorhinolaryngology, Seoul National University Hospital, Seoul, Korea. drmung@naver.com
Abstract
OBJECTIVES
Rectified vestibular evoked myogenic potential (rVEMP) is new method that simultaneously measures the muscle contraction power during VEMP recordings. Although there are a few studies that have evaluated the effect of the rVEMP, there is no study that has evaluated the capacity of rVEMP during asymmetrical muscle contraction.
METHODS
Thirty VEMP measurements were performed among 20 normal subjects (mean age, 28.2+/-2.1 years; male, 16). VEMP was measured in the supine position. The head was turned to the right side by 0degrees, 15degrees, 30degrees, and 45degrees and the VEMPs were recorded in each position. The interaural amplitude difference (IAD) ratio was calculated by the conventional non-rectified VEMP (nVEMP) and rVEMP.
RESULTS
The nVEMP IAD increased significantly according to increasing neck rotation. The IAD in rVEMP was almost similar from 0degrees to 30degrees. However, the IAD was significantly larger than the other positions when the neck was rotated 45degrees. When IAD during 0degrees was set as a standard, the IAD of the rVEMP was significantly smaller that the nVEMP only during the 30degrees rotaion.
CONCLUSION
Rectified VEMP is capable of correcting asymmetrical muscle contraction power. In contrast, it cannot correct the asymmetry if muscle contraction power asymmetry is 44.8% or larger. Also, it is not necessary if muscle contraction power asymmetry is 22.5% or smaller.
Keyword
MeSH Terms
Figure
-

Fig. 1 Position of the subject to induce asymmetric muscle contraction. First, the ceiling was marked for 0°, 15°, 30°, and 45° rotations. The vestibular evoked myogenic potential (VEMP) was measured in the supine position while the head was elevated 2 cm from the bed. The head was then turned towards the right at 0°, 15°, 30°, and 45°. The VEMP was recorded in each position.
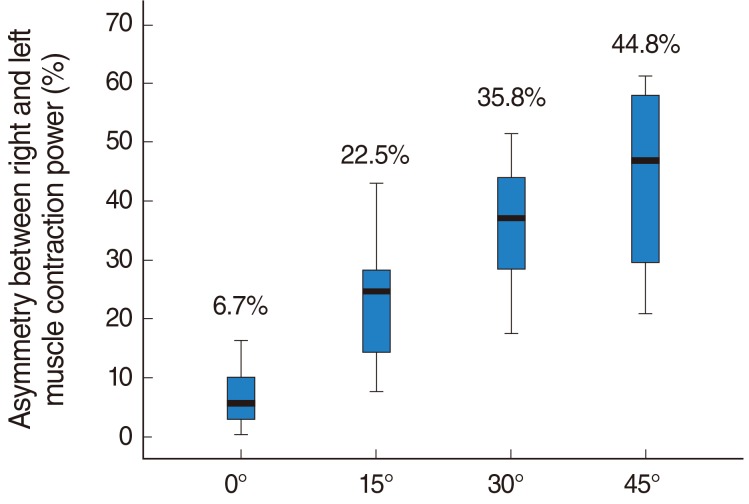
Fig. 2 Asymmetry between right and left muscle contraction power. The asymmetry of muscle contraction power increased in a linear pattern as the head was turned more towards the right side. This difference was quantified with the following formula: muscle contraction power asymmetry (%)=(left muscle contraction power-right muscle contraction power)/(left muscle contraction power+right muscle contraction power)×100.

Fig. 3 Interaural amplitude difference (IAD). The IAD of non-rectified conventional vestibular evoked myogenic potential (nVEMP) increased as the head rotation angle increased but plateaued at 30° and 45° (A). IAD during asymmetric muscle contraction (15°, 30°, and 45°) was significantly different from the 0° condition. The IAD of rectified VEMP (rVEMP) was stable with minimal differences from 0° to 30°, but significantly increased at 45° (B).
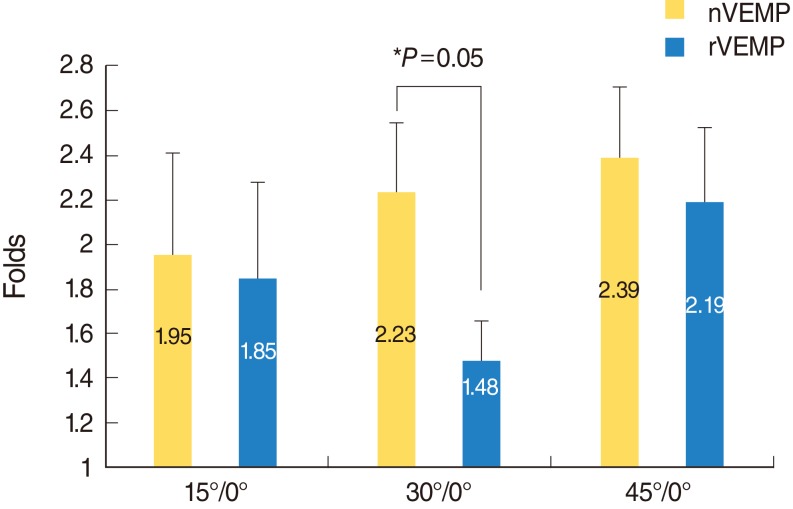
Fig. 4 Relative increase in interaural amplitude difference ratio (ΔIAD). In order to quantify the perturbation of IAD solely due to asymmetric muscle contraction, the IAD at 15°, 30°, and 45° was compared with that at the 0° condition. The ratio of IAD at each position relative to 0° was expressed as ΔIAD (ΔIAD=IAD at each position / 0° IAD). The ΔIAD of rectified conventional VEMP was significantly smaller than that of the non-rectified conventional VEMP at 30°. VEMP, vestibular evoked myogenic potential.
Reference
-
1. Suh MW, Jeong SH, Kim JS. Vestibular evoked myogenic potential: recording methods and clinical application. J Korean Neurol Assoc. 2010; 2. 28(1):1–12.2. Colebatch JG, Halmagyi GM, Skuse NF. Myogenic potentials generated by a click-evoked vestibulocollic reflex. J Neurol Neurosurg Psychiatry. 1994; 2. 57(2):190–197. PMID: 8126503.
Article3. Lim CL, Clouston P, Sheean G, Yiannikas C. The influence of voluntary EMG activity and click intensity on the vestibular click evoked myogenic potential. Muscle Nerve. 1995; 10. 18(10):1210–1213. PMID: 7659119.
Article4. Ochi K, Ohashi T, Nishino H. Variance of vestibular-evoked myogenic potentials. Laryngoscope. 2001; 3. 111(3):522–527. PMID: 11224786.
Article5. Suh MW, Kim JS, Koo JW. Influence of blood pressure manometer feedback on the parameters of the vestibular evoked myogenic potential test. Ann Otol Rhinol Laryngol. 2009; 4. 118(4):281–286. PMID: 19462849.
Article6. Vanspauwen R, Wuyts FL, Van De Heyning PH. Validity of a new feedback method for the VEMP test. Acta Otolaryngol. 2006; 8. 126(8):796–800. PMID: 16846920.
Article7. Lee KJ, Kim MS, Son EJ, Lim HJ, Bang JH, Kang JG. The usefulness of rectified VEMP. Clin Exp Otorhinolaryngol. 2008; 9. 1(3):143–147. PMID: 19434246.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predictive Value of Rectified Vestibular Evoked Myogenic Potential in Determining Lesion Side in Unilateral Vestibulopathy Patients
- Clinical Application and Updates on Vestibular Evoked Myogenic Potential: Proposal for Future Development in Vestibulopathy
- The Usefulness of Rectified VEMP
- The Principle and Methodology of Vestibular Evoked Myogenic Potential
- Preserved Ocular Vestibular Evoked Myogenic Potential to Head Tap in a Patient with Positive Head-Heave
