Coexistence of a Carotid Body Tumor and Thyroglossal Duct Carcinoma With Cervical Lymph Node Metastasis
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, Seoul, Korea.
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 3Department of Radiology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 4Department of Pathology, Soonchunhyang University College of Medicine, Bucheon, Korea.
- 5Department of Otorhinolaryngology, Yonsei University College of Medicine, Seoul, Korea. ywkohent@yuhs.ac
Abstract
- Thyroglossal duct carcinoma is uncommon, occurring in approximately 1% of all thyroglossal duct remnants. This rare neoplasm is characterized by relatively nonaggressive behavior with infrequent lymph nodal spread. Another rare neoplasm of the head and neck region is a carotid body tumor. A 78-year-old woman with a 3-year history of midline and bilateral neck masses was referred to us. Fine needle aspiration biopsies and a computed tomography scan suggested the diagnosis of thyroglossal duct carcinoma with cervical lymph node metastasis. Interestingly, the left-side neck mass was found to be splaying the carotid bifurcation, on computed tomography imaging. Carotid arteriography demonstrated a highly vascular mass in the bifurcation of the carotid artery that was compressing the internal and external carotid arteries. To our knowledge, this is the first reported instance of a thyroglossal duct carcinoma with neck metastasis accompanied by a carotid body tumor. In addition, the carotid body tumor in this case mimicked neck metastasis from the thyroglossal duct carcinoma.
MeSH Terms
Figure
-
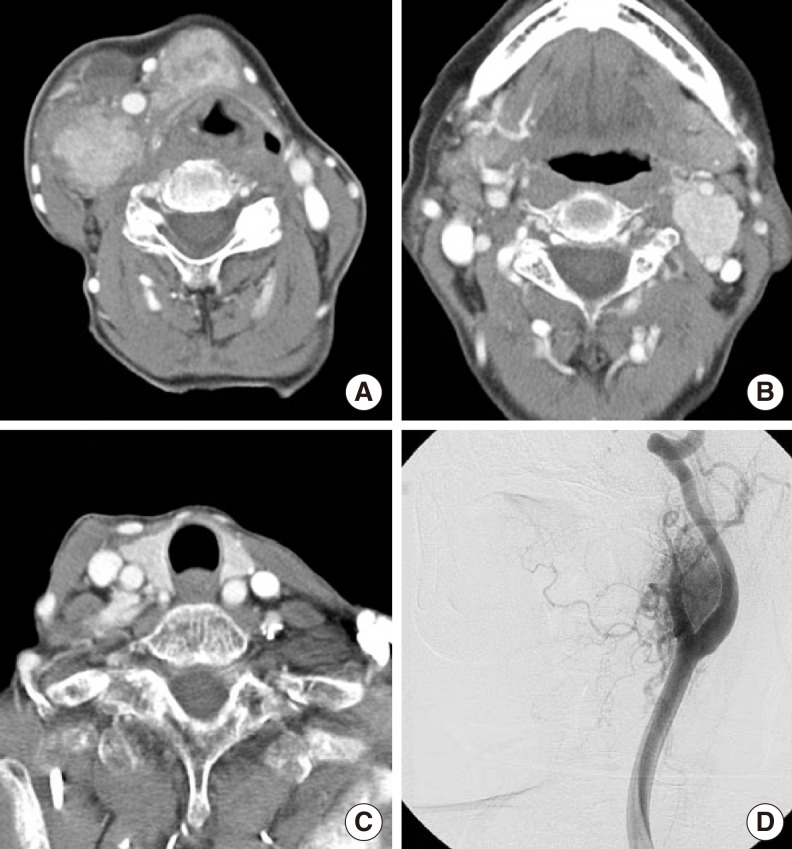
Fig. 1 Axial view of a computed tomography scan with contrast showing a round heterogeneously enhanced mass with irregular margins at the level of the hyoid bone with multiple enhanced, enlarged cervical lymph nodes on the right, at level II (A). Note that a highly enhanced mass was located at the carotid bifurcation (B). There was no abnormal lesion in the thyroid gland (C). Carotid arteriography demonstrated a highly vascular mass at the bifurcation of the carotid artery that was compressing the internal and external carotid arteries (D).
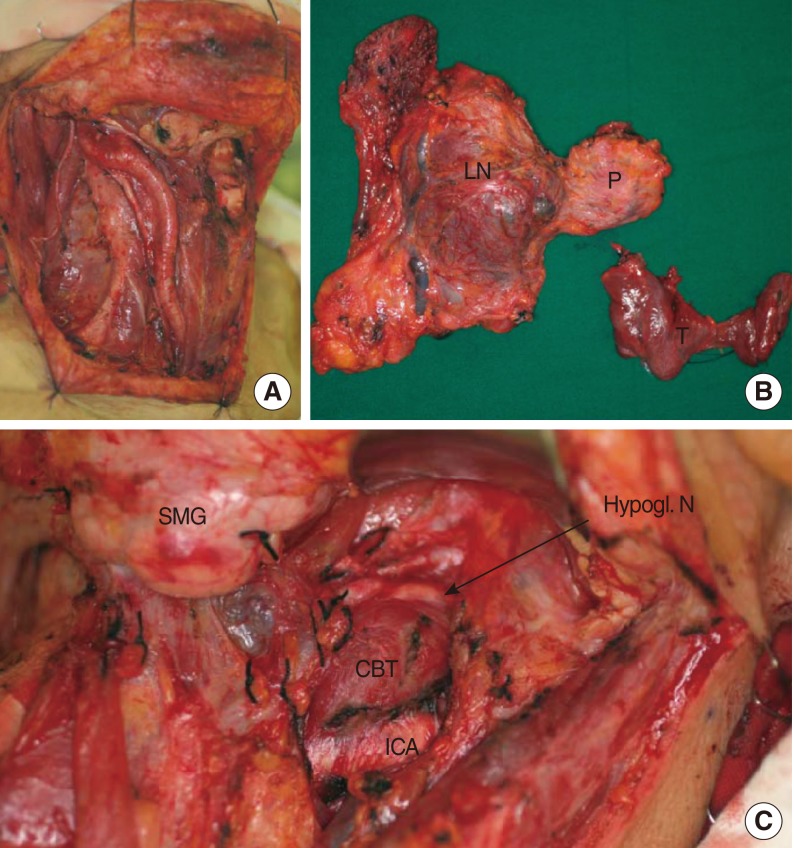
Fig. 2 Photograph of the intraoperative findings showing the surgical field of the right side of the neck after the completion of modified neck dissection (A). Surgical specimens showing the en bloc specimen of the neck dissection and thyroglossal duct carcinoma and total thyroidectomy specimen (B). Note that the CBT was located between the internal and external arteries, splaying the carotid bifurcation (C). P, primary tumor; LN, metastatic lymph nodes; T, thyroid gland; SMG, submandibular gland; CBT, carotid body tumor; ICA, internal carotid artery; Hypogl. N, hypoglossal nerve.
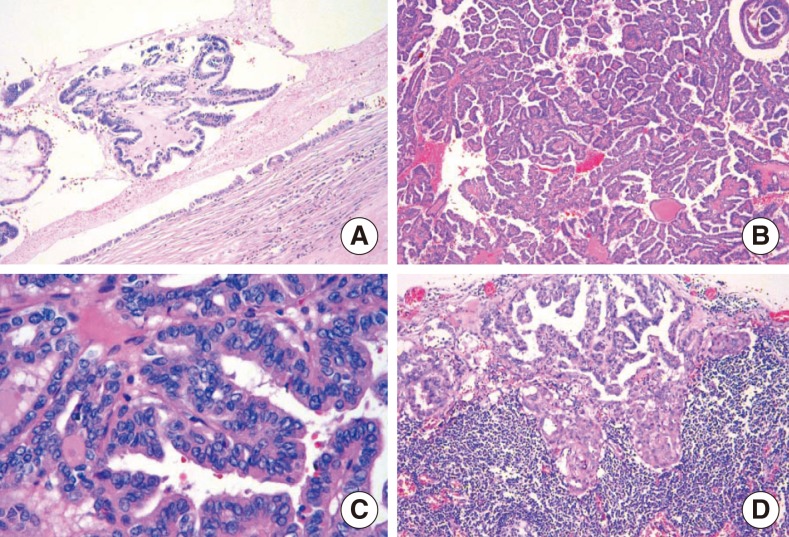
Fig. 3 Histopathologic findings. A thyroglossal duct cyst lined by a single row of columnar epithelium (H&E, ×40) (A). The tumor was composed of small and large papillary structures with fibrovascular cores (H&E, ×100) (B). The tumor cells lining the papillary structures showed nuclear grooves and nuclear clearing, which are characteristic nuclear features of papillary thyroid carcinoma. The nuclei showed a thick, irregular nuclear membrane, a high nuclear/cytoplasmic ratio, and somewhat eccentric nucleoli (H&E, ×400) (C). A lymph node showing subcapsular sinusoidal metastatic carcinoma. The histological appearance of the metastatic carcinoma is the same as that of the primary tumor (H&E, ×100) (D).
Reference
-
1. Boswell WC, Zoller M, Williams JS, Lord SA, Check W. Thyroglossal duct carcinoma. Am Surg. 1994; 9. 60(9):650–655. PMID: 8060034.2. Weiss SD, Orlich CC. Primary papillary carcinoma of a thyroglossal duct cyst: report of a case and literature review. Br J Surg. 1991; 1. 78(1):87–89. PMID: 1998873.
Article3. Plaza CP, Lopez ME, Carrasco CE, Meseguer LM, Perucho Ade L. Management of well-differentiated thyroglossal remnant thyroid carcinoma: time to close the debate? Report of five new cases and proposal of a definitive algorithm for treatment. Ann Surg Oncol. 2006; 5. 13(5):745–752. PMID: 16538412.
Article4. Lack EE, Cubilla AL, Woodruff JM, Farr HW. Paragangliomas of the head and neck region: a clinical study of 69 patients. Cancer. 1977; 2. 39(2):397–409. PMID: 837327.5. Netterville JL, Reilly KM, Robertson D, Reiber ME, Armstrong WB, Childs P. Carotid body tumors: a review of 30 patients with 46 tumors. Laryngoscope. 1995; 2. 105(2):115–126. PMID: 8544589.
Article6. Miccoli P, Minuto MN, Galleri D, Puccini M, Berti P. Extent of surgery in thyroglossal duct carcinoma: reflections on a series of eighteen cases. Thyroid. 2004; 2. 14(2):121–123. PMID: 15068626.
Article7. Branstetter BF, Weissman JL, Kennedy TL, Whitaker M. The CT appearance of thyroglossal duct carcinoma. AJNR Am J Neuroradiol. 2000; 9. 21(8):1547–1550. PMID: 11003294.8. Samara C, Bechrakis I, Kavadias S, Papadopoulos A, Maniatis V, Strigaris K. Thyroglossal duct cyst carcinoma: case report and review of the literature, with emphasis on CT findings. Neuroradiology. 2001; 8. 43(8):647–649. PMID: 11548172.
Article9. Widstrom A, Magnusson P, Hallberg O, Hellqvist H, Riiber H. Adenocarcinoma originating in the thyroglossal duct. Ann Otol Rhinol Laryngol. 1976; Mar-Apr. 85(2 pt 1):286–290. PMID: 1267333.
Article10. Albores-Saavedra J, Duran ME. Association of thyroid carcinoma and chemodectoma. Am J Surg. 1968; 12. 116(6):887–890. PMID: 4302028.
Article11. Larraza-Hernandez O, Albores-Saavedra J, Benavides G, Krause LG, Perez-Merizaldi JC, Ginzo A. Multiple endocrine neoplasia: pituitary adenoma, multicentric papillary thyroid carcinoma, bilateral carotid body paraganglioma, parathyroid hyperplasia, gastric leiomyoma, and systemic amyloidosis. Am J Clin Pathol. 1982; 10. 78(4):527–532. PMID: 7137085.
Article12. Kuratomi Y, Kumamoto Y, Sakai Y, Komiyama S. Carotid body tumor associated with differentiated thyroid carcinoma. Eur Arch Otorhinolaryngol. 1994; 251(Suppl 1):S91–S94. PMID: 11894786.
Article13. Luna-Ortiz K, Hurtado-Lopez LM, Valderrama-Landaeta JL, Ruiz-Vega A. Thyroglossal duct cyst with papillary carcinoma: what must be done? Thyroid. 2004; 5. 14(5):363–366. PMID: 15186613.
Article14. Rush BF Jr. Current concepts in the treatment of carotid body tumors. Surgery. 1962; 10. 52:679–684. PMID: 14495345.15. O'Connell M, Grixti M, Harmer C. Thyroglossal duct carcinoma: presentation and management, including eight cases reports. Clin Oncol (R Coll Radiol). 1998; 10(3):186–190. PMID: 9704182.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Papillary Carcinoma Arising in Thyroglossal Duct Cyst: A Case Report
- Thyroid Cancer Arising from Thyroglossal Duct Cyst
- Primary Papillary Carcinoma Arising in a Thyroglossal Duct Cyst
- A Case of Papillary Carcinoma in Thyroglossal Duct Cyst with Mandibular Invasion
- Pattern of Cervical Neck Lymph Node Metastasis in Papillary Thyroid Carcinoma according to Tumor Size
