Korean J Obstet Gynecol.
2011 Nov;54(11):731-735. 10.5468/KJOG.2011.54.11.731.
Parasitic myoma in mesentery mimicking gastrointestinal stromal tumor: A case of laparoscopic myomectomy with single port approach
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. ds123.bae@samsung.com
- KMID: 2274116
- DOI: http://doi.org/10.5468/KJOG.2011.54.11.731
Abstract
- Gastrointestinal stromal tumor (GIST) is the most common non-epithelial tumor in the gastrointestinal tract, and express a highly specific marker called c-kit (CD117). The majorinty of GISTs arise in the stomach (60%) and small bowel (30%), and remaining 10% in the other gastrointestinal tract. It also occurs, rarely, in non-gastrointestinal tract. We experienced a 42-year-old woman who was transferred to our hospital with the impression of GIST by positron emission tomography-computed tomography, and after the single port approach laparoscopy, finally diagnosed as parasitic myoma. Hysterectomy and complete resection of 14cm sized mesenteric mass was done via single port laparoscopy. After the immunohistochemistry test, the final pathologic diagnosis was confirmed the diagnosis of myoma. We report here the case of parasitic myoma mimicking GIST with brief review of articles.
MeSH Terms
Figure
-
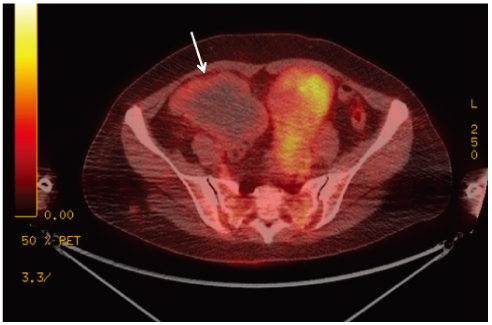
Fig. 1 Irregular shaped mass (white arrow) with central necrosis and high fludeoxyglucose uptake in the periphery is found in the right pelvic cavity and the size of tumor was about 12 cm in longest diameter in preoperative positron emission tomography-computed tomography scan.
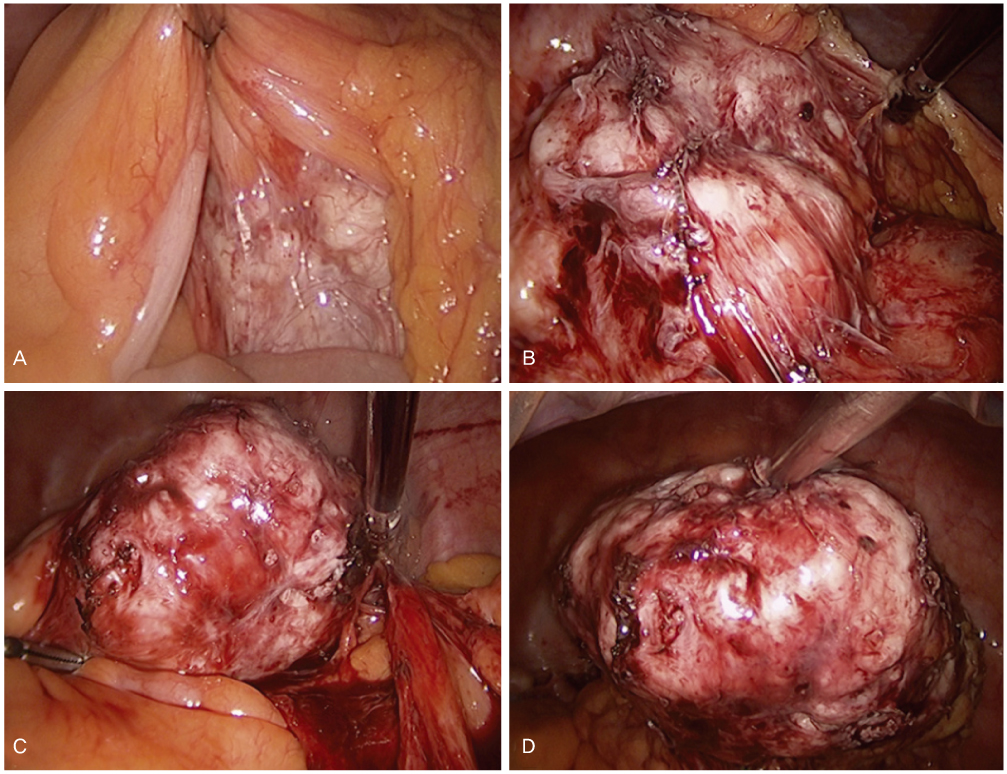
Fig. 2 Under laparoscopic evaluation, the mass is located under the mesentery of the colon and small intestines with adhesion.

Fig. 3 The tumor is formed by interlacing bundles of smooth muscle cells with multifocal hyaline degeneration. There is no pleomorphism, atypia or excessive mitotic figures (H&E, ×100).
Reference
-
1. Machairas A, Karamitopoulou E, Tsapralis D, Karatzas T, Machairas N, Misiakos EP. Gastrointestinal stromal tumors (GISTs): an updated experience. Dig Dis Sci. 2010. 55:3315–3327.2. Kang YK, Kim KM, Sohn T, Choi D, Kang HJ, Ryu MH, et al. Clinical practice guideline for accurate diagnosis and effective treatment of gastrointestinal stromal tumor in Korea. J Korean Med Sci. 2010. 25:1543–1552.3. Blay JY, von Mehren M, Blackstein ME. Perspective on updated treatment guidelines for patients with gastrointestinal stromal tumors. Cancer. 2010. 116:5126–5137.4. Fasih N, Prasad Shanbhogue AK, Macdonald DB, Fraser-Hill MA, Papadatos D, Kielar AZ, et al. Leiomyomas beyond the uterus: unusual locations, rare manifestations. Radiographics. 2008. 28:1931–1948.5. Kho KA, Nezhat C. Parasitic myomas. Obstet Gynecol. 2009. 114:611–615.6. Larraín D, Rabischong B, Khoo CK, Botchorishvili R, Canis M, Mage G. "Iatrogenic" parasitic myomas: unusual late complication of laparoscopic morcellation procedures. J Minim Invasive Gynecol. 2010. 17:719–724.7. Moon HS, Koo JS, Park SH, Park GS, Choi JG, Kim SG. Parasitic leiomyoma in the abdominal wall after laparoscopic myomectomy. Fertil Steril. 2008. 90:1201.e1–1201.e2.8. Nezhat C, Kho K. Iatrogenic myomas: new class of myomas? J Minim Invasive Gynecol. 2010. 17:544–550.9. Yeh HC, Kaplan M, Deligdisch L. Parasitic and pedunculated leiomyomas: ultrasonographic features. J Ultrasound Med. 1999. 18:789–794.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Parasitic Leiomyoma with Lymphatic Dilatation in Trocar Port-Site of Abdominal Wall: A Case Report
- The usefulness of laparoscopic myomectomy after Hormone Replacement Therapy in postmenopausal women with uterine myoma
- Extragastrointestinal Stromal Tumor Mimicking Gastric Subepithelial Tumor
- Surgical outcomes for robot-assisted laparoscopic myomectomy compared with laparoscopic myomectomy
- Hybrid laparoscopic myomectomy: A novel technique
