Application and effects of condylectomy in asymmetric patients with condylar hyperplasia
- Affiliations
-
- 1Department of Orthodontics, School of Dentistry, Yonsei University, Korea.
- 2Department of Orthodontics, School of Dentistry, Yonsei University, Dental Science Research Institute, Korea. hwang@yuhs.ac
- KMID: 2273975
- DOI: http://doi.org/10.4041/kjod.2008.38.6.437
Abstract
- Condylar hyperplasia is a pathologic condition showing 3-dimensional skeletal hyperplasia of the mandible. The reason for condylar hyperplasia is not yet known, but the effects of hormone, trauma, infection, genetics, fetal condition, and hypervascularity are known as possible reasons. When we diagnose a patient as having condylar hyperplasia, it is important to decide if it is in progress or not. Treatment for facial asymmetry due to condylar hyperplasia are decided accordingly, including condylectomy, that is removal of growth site of the affected condyle, and conventional orthognathic surgery only or condylectomy with orthognathic surgery after the completion of growth. Therefore, it is important to determine the growth state of condylar hyperplasia in treatment stability. This is verified through bone scan and regular check-ups with 3D CT or PA cephalogram. This case report introduces an improved case of facial asymmetry with condylectomy together with orthognathic surgery.
Figure
-
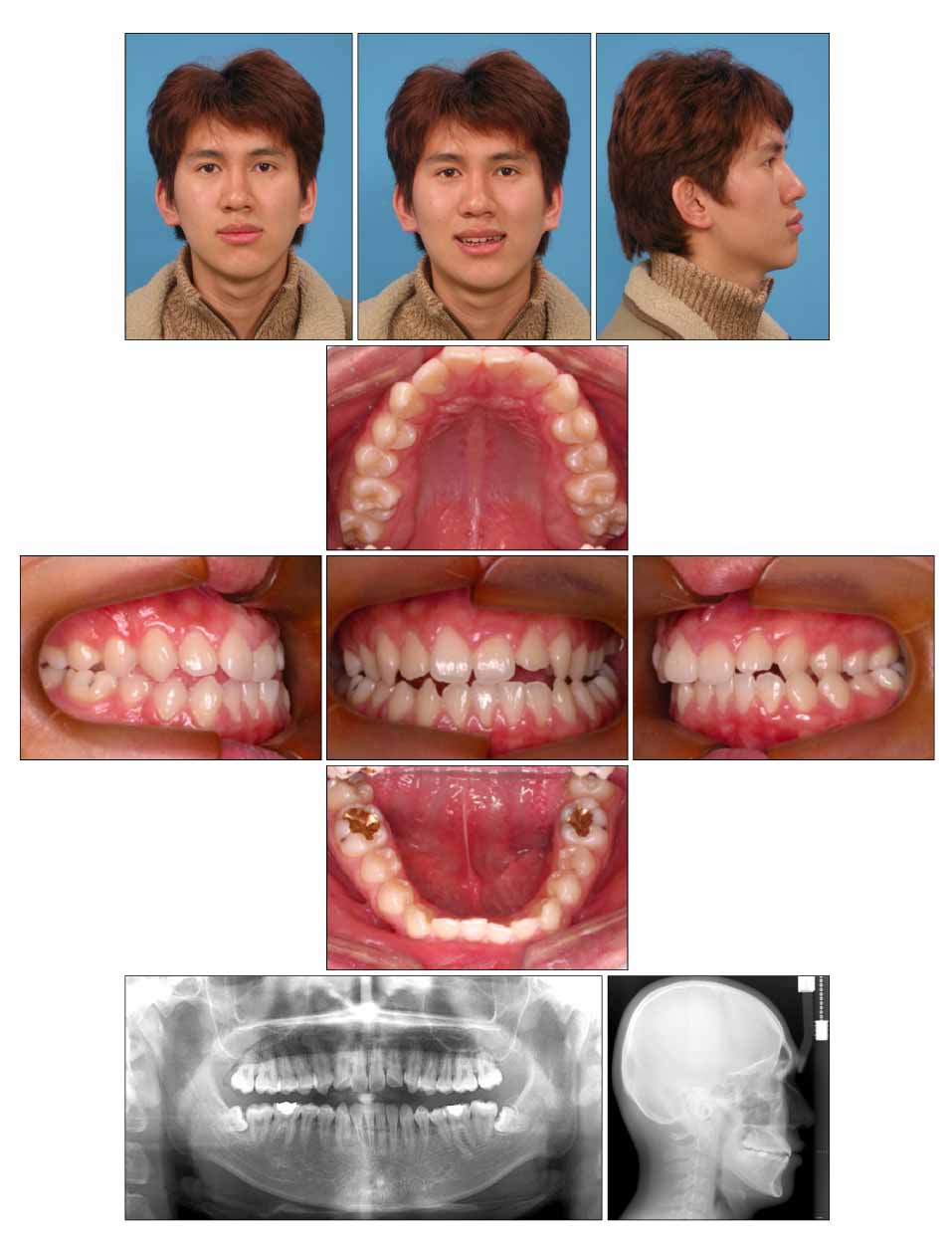
Fig 1 Facial and intraoral photographs and panoramic and cephalometric radiographs before treatment.
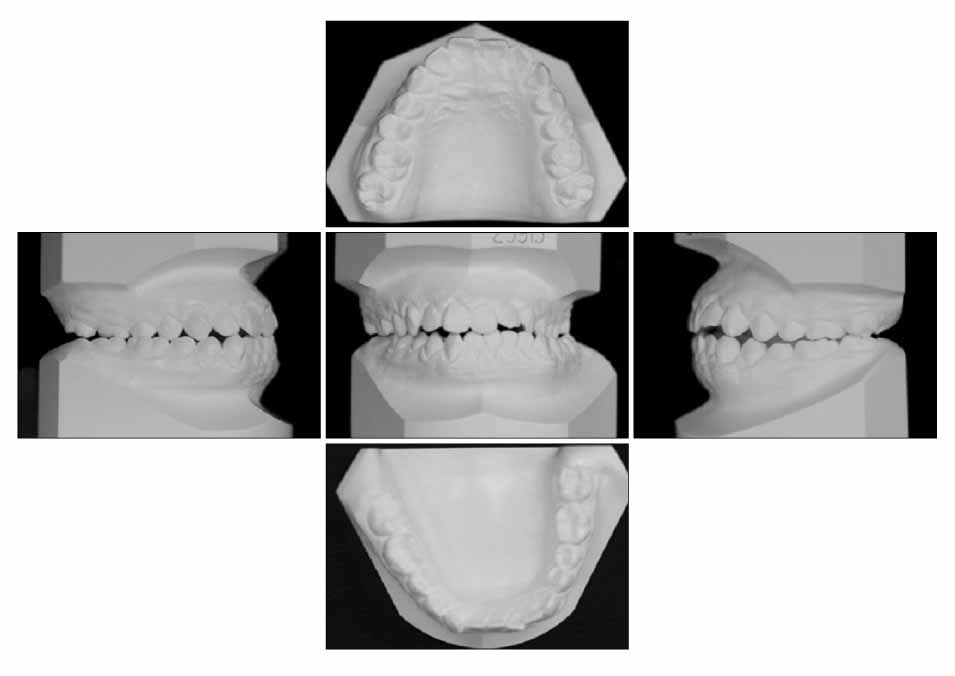
Fig 2 Cast analysis before treatment. There is a mandibular midline deviation of 12.0 mm to the left side and the mandibular arch is asymmetric.
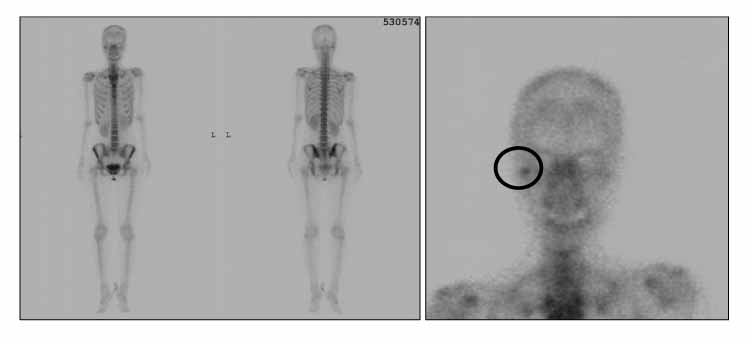
Fig 3 Bone scan results for case 1. Radio-isotope uptake was increased in the right condylar process area.
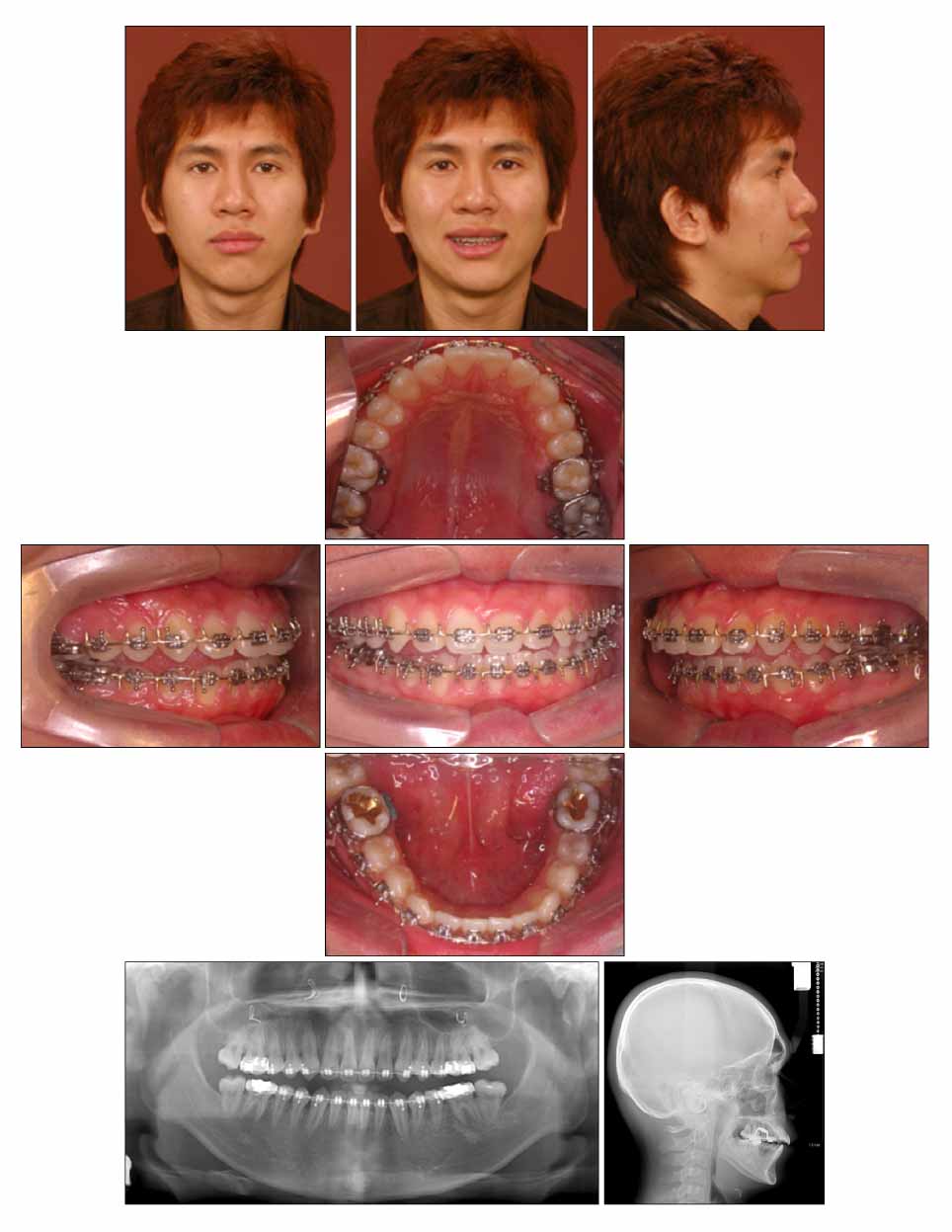
Fig 4 Facial and intraoral photographs and panoramic and cephalometric radiographs after condylectomy for case 1.
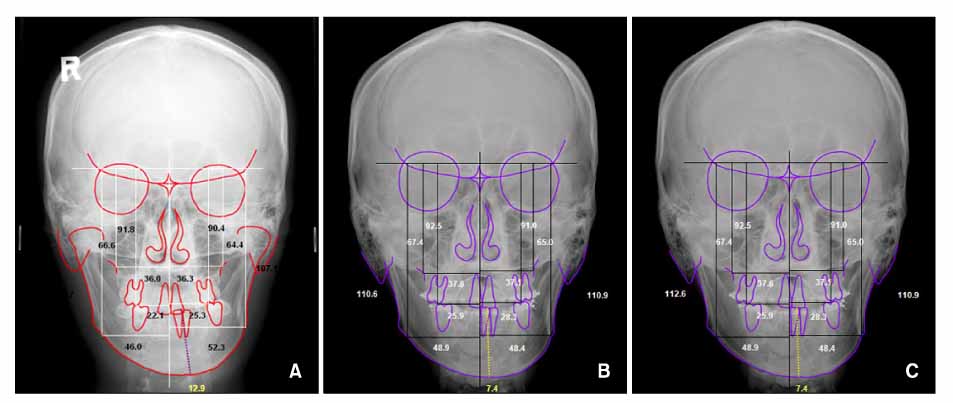
Fig 5 Posterior-Anterior cephalogram for case 1. A, Before treatment; B, after condylectomy; C, after treatment.
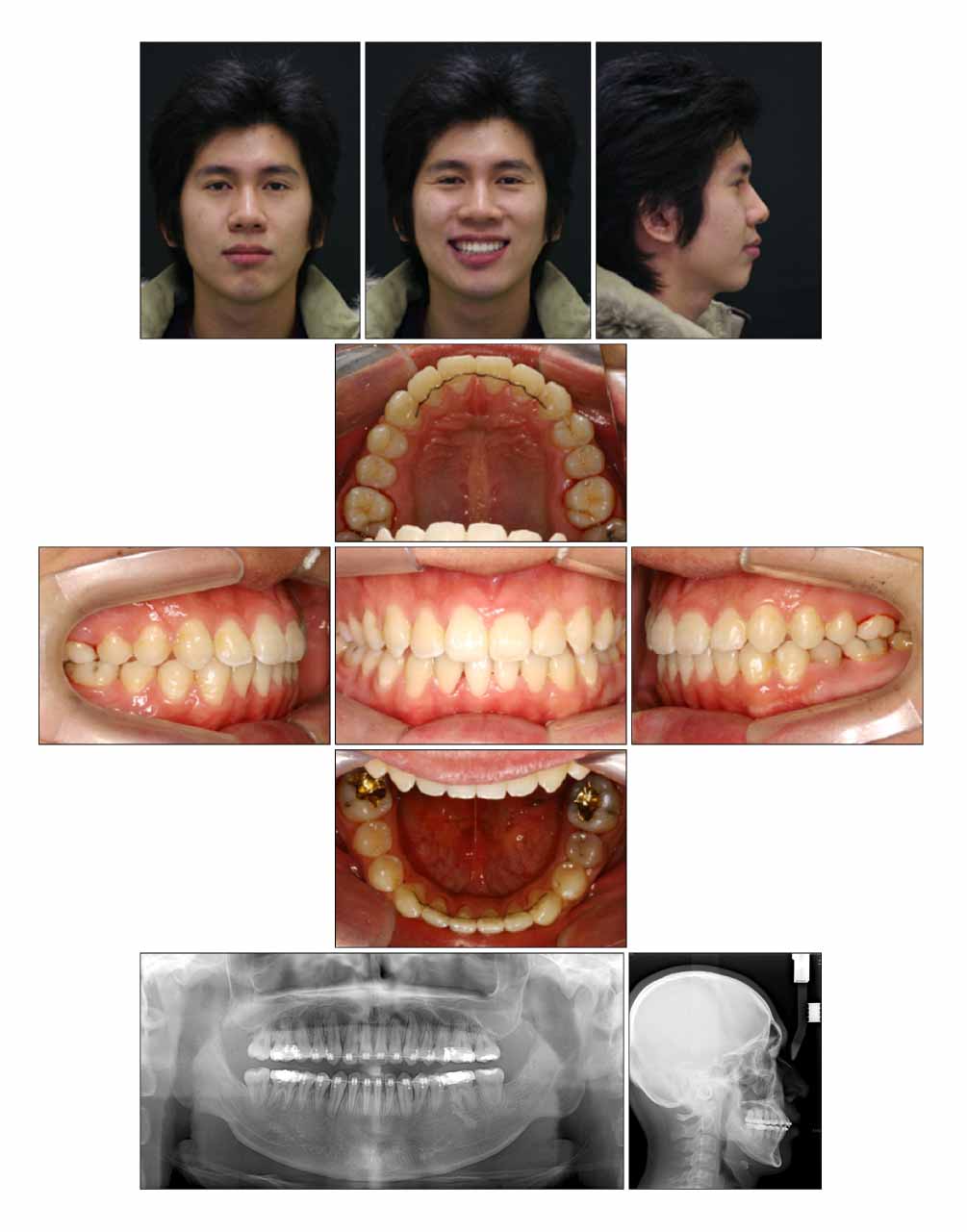
Fig 6 Facial and intraoral photographs and panoramic and cephalometric radiographs after condylectomy for case 1.
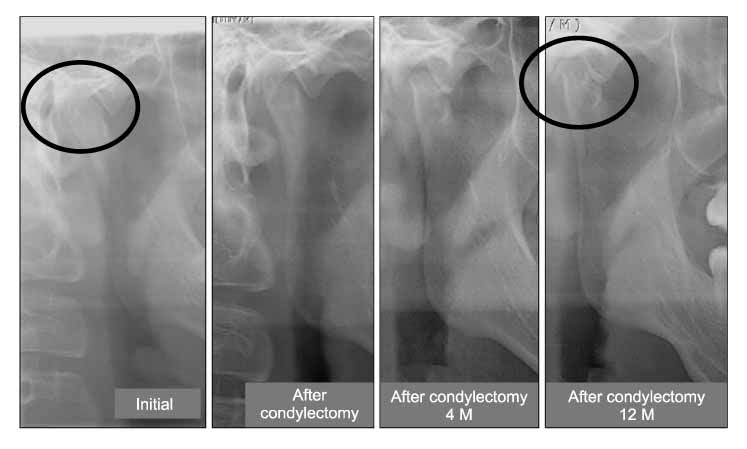
Fig 7 Progressive condyle remodeling on panoramic x-ray for case 1. Four months after condylectomy, twelve months after condylectomy there was a continuous cortical layer on the left condyle. Resected condyle was remodeled in the new position.
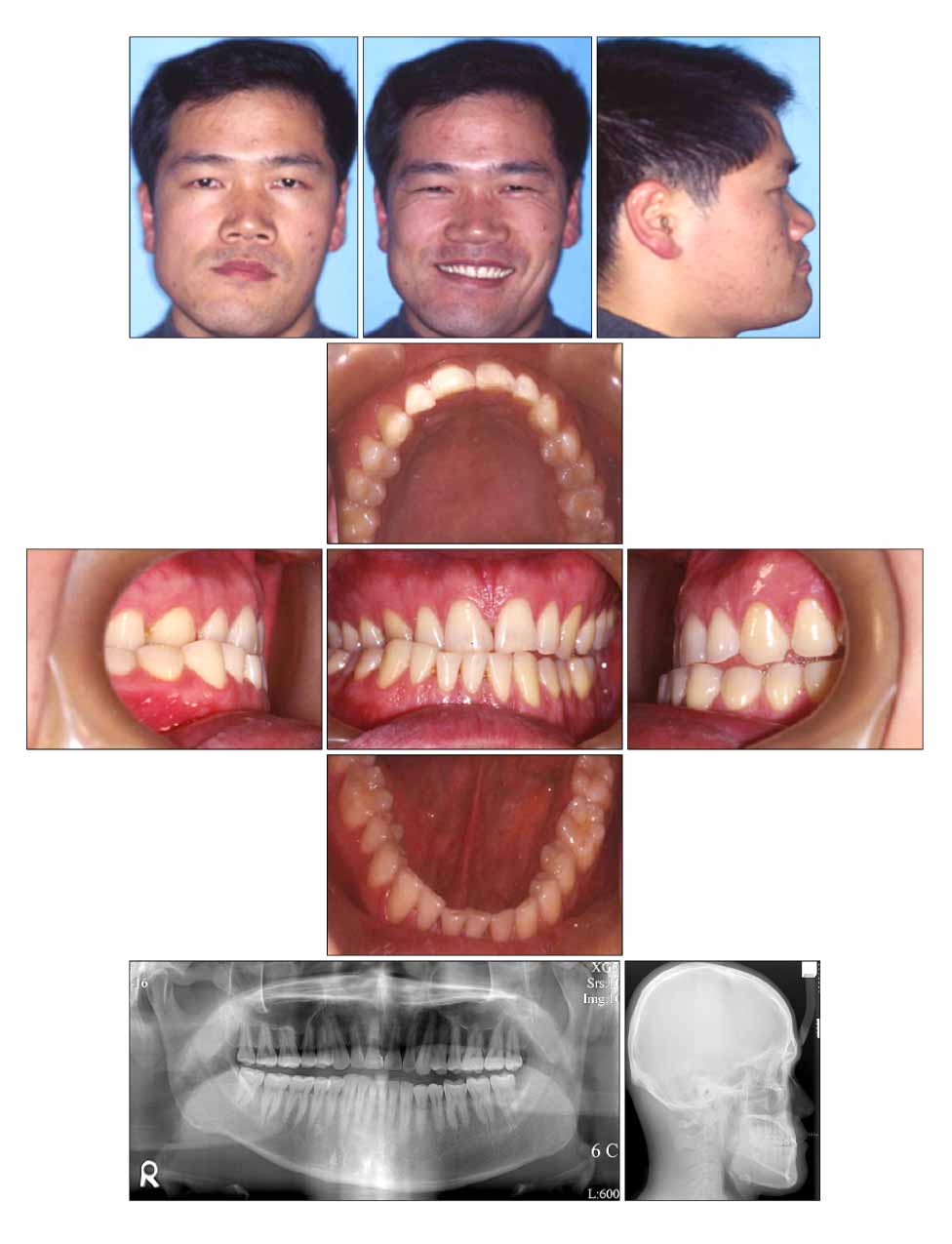
Fig 8 Facial and intraoral photographs and panoramic and cephalometric radiographs before treatment for case 2.

Fig 9 Cast analysis before treatment for case 2. It shows mandibular midline deviation of 14.0 mm. There is an occlusal canting with the left side more caudal than the right side.
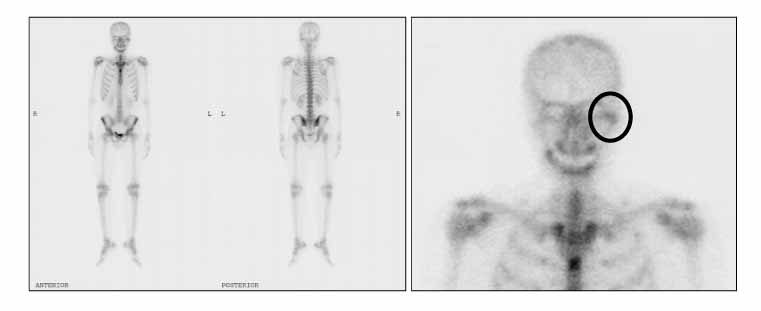
Fig 10 Bone scan results for case 2. Radio-isotope uptake was increased on the left condylar process area.
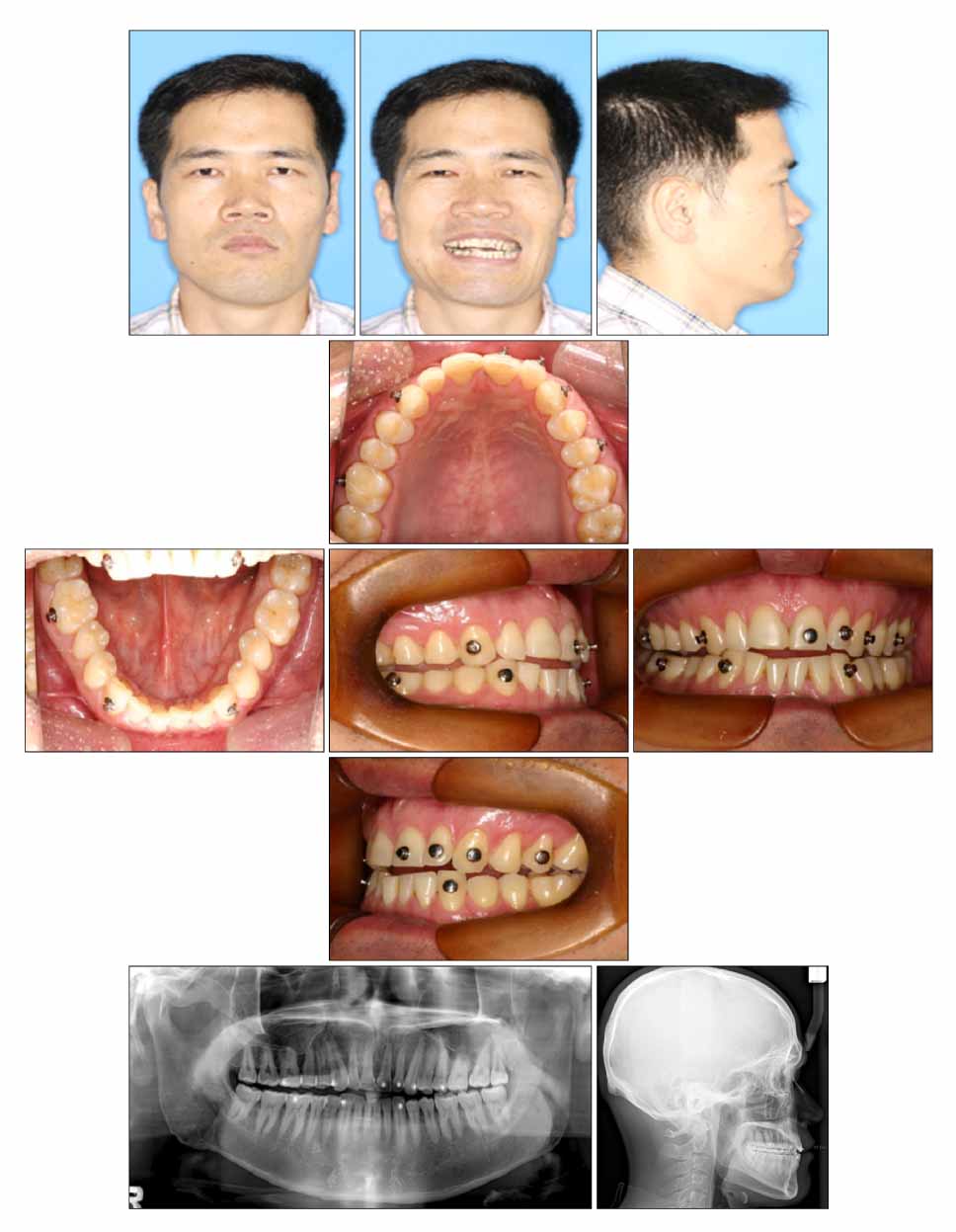
Fig 11 Facial and intraoral photographs and panoramic and cephalometric radiographs after condylectomy for case 2.

Fig 12 Intraoral photograph for molar intrusion and torque control for case 2. Four miniscrews were inserted to intrude molars on the left maxilla buccal and palatal area and a multi loop was used to add buccal crown torque to the right maxilla area.

Fig 13 Facial and intraoral photographs and panoramic and cephalometric radiographs after treatment for case 2.
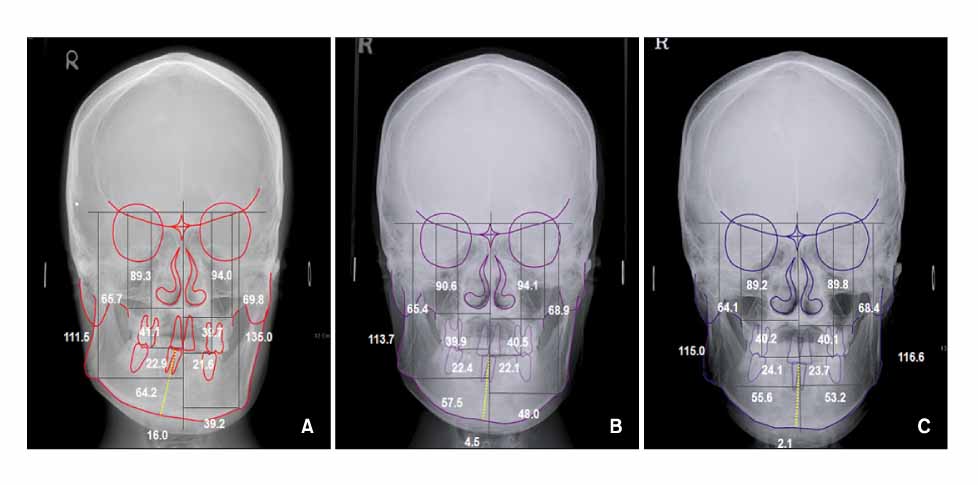
Fig 14 Posterior-Anterior cephalogram for case 2. A, Before treatment; B, after condylectomy; C, after treatment.
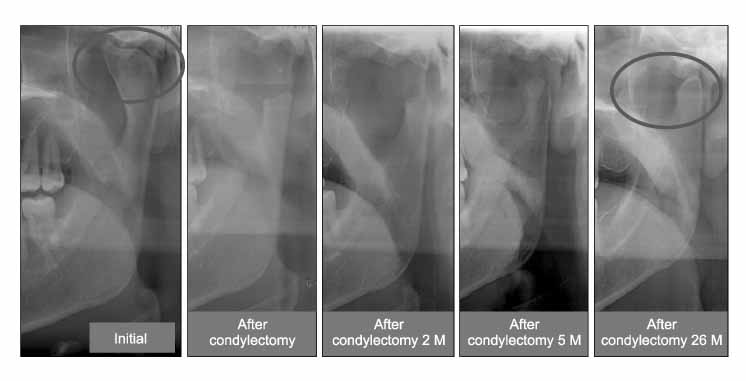
Fig 15 After condylectomy, resected condyle was remodeled in the new position. After five months, condylar shape is getting smoothly rounded, and twenty six months later, it was remodeled to a normal condylar shape.
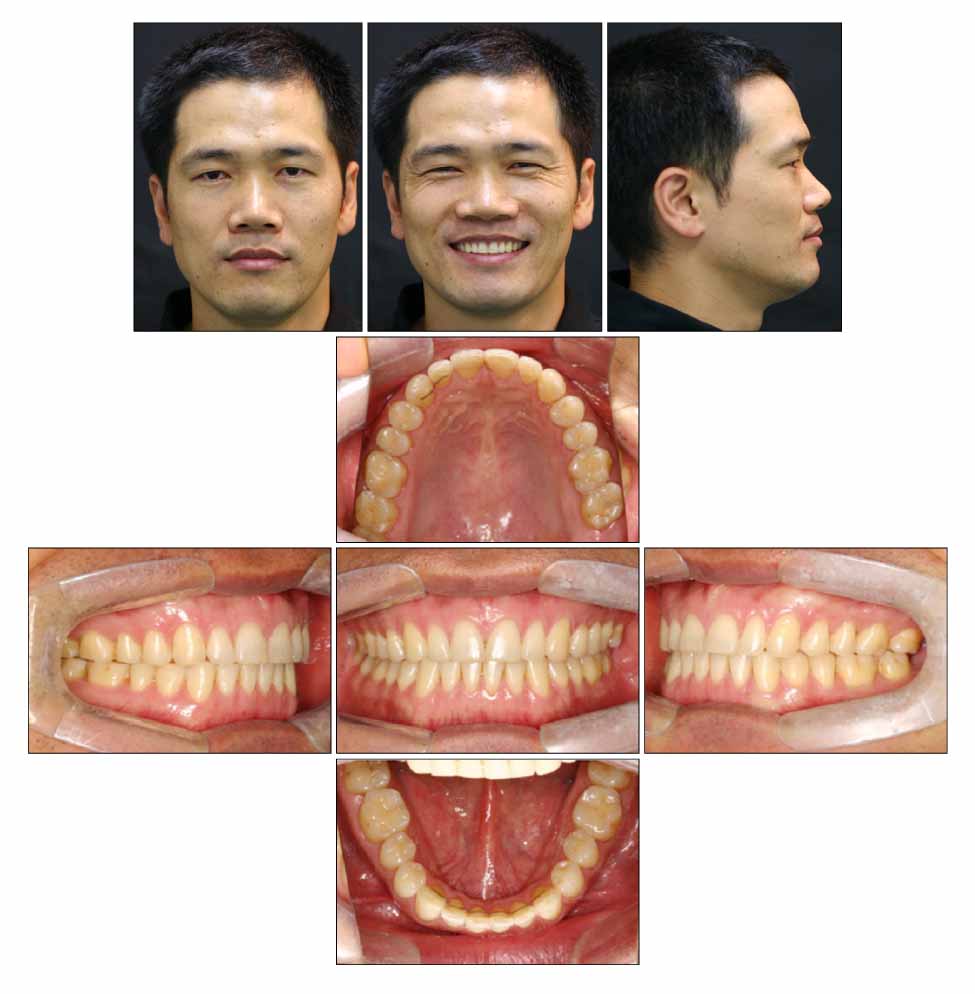
Fig 16 Facial and intraoral photographs after 9 months of treatment for case 2.

Fig 17 Principles of condylar hyperplasia treatment. The most important factor to decide is whether the condyle is growing or not to treat the facial asymmetry due to condylar hyperplasia.
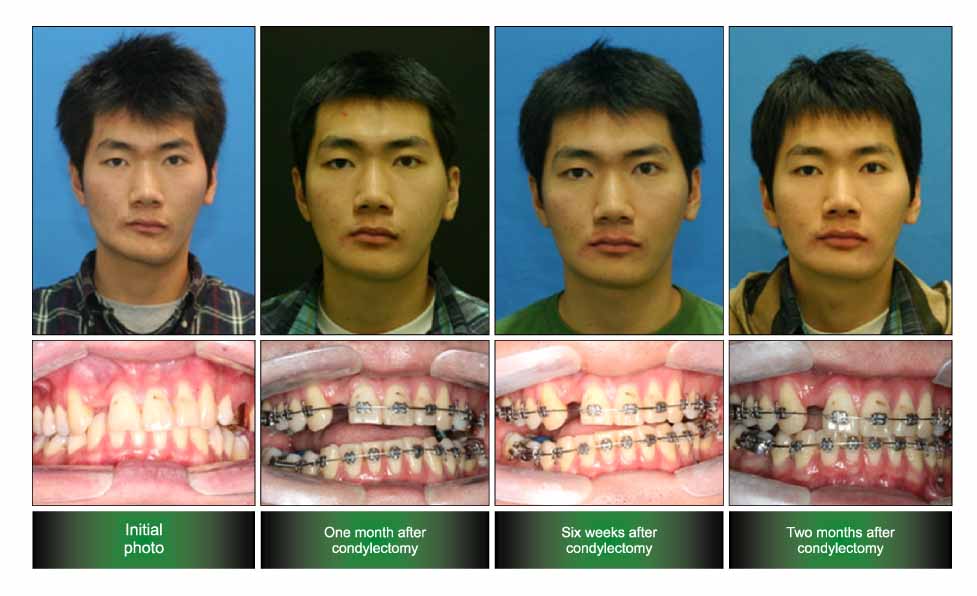
Fig 18 Clinical healing pattern after condylectomy. Straight after condylectomy, there is lateral openbite on the unaffected side. According to the remodeling process, lateral openbite is closed and facial asymmetry is improved.

Fig 19 Superimposition of cephalometric tracing of before treatment and after condylectomy (Red: before treatment, Blue: after condylectomy). Molar was intruded and alveolar area was remodeled on the affected area (left side). But there were no changes in the maxillary basal bone area.
Reference
-
1. Chen YR, Bender-Samuel RL, Huang CS. Hemimandibular hyperplasia. Plast Reconstr Surg. 1996. 97:730–737.
Article2. Hampf G, Tasanen A, Nordling S. Surgery in mandibular condylar hyperplasia. J Maxillofac Surg. 1985. 13:74–78.
Article3. Iannetti G, Cascone P, Belli E, Cordaro L. Condylar hyperplasia: cephalometric study, treatment planning, and surgical correction (our experience). Oral Surg Oral Med Oral Pathol. 1989. 68:673–681.
Article4. Bishara SE, Burkey PS, Kharouf JG. Dental and facial asymmetries: a review. Angle Orthod. 1994. 64:89–98.5. Burstone CJ. Diagnosis and treatment planning of patients with asymmetries. Semin Orthod. 1998. 4:153–164.6. Nitzan DW, Katsnelson A, Bermanis I, Brin I, Casap N. The clinical characteristics of condylar hyperplasia: experience with 61 patients. J Oral Maxillofac Surg. 2008. 66:312–318.
Article7. Betts NJ, Vanarsdall RL, Barber HD, Higgins-Barber K, Fonseca RJ. Diagnosis and treatment of transverse maxillary deficiency. Int J Adult orthodon Orthognath Surg. 1995. 10:75–96.8. Araz B, Nitzan DW, Brin I. Condylar hyperplasia: remodeling of facial structures following condylectomy. Report of two cases. Int J Adult Orthodon Orthognath Surg. 1991. 6:47–55.9. Hodder SC, Rees JI, Oliver TB, Facey PE, Sugar AW. SPECT bone scintigraphy in the diagnosis and management of mandibular condylar hyperplasia. Br J Oral Maxillofac Surg. 2000. 38:87–93.
Article10. Henderson MJ, Wastie ML, Bromige M, Selwyn P, Smith A. Technetium-99m bone scintigraphy and mandibular condylar hyperplasia. Clin Radiol. 1990. 41:411–414.
Article11. Miyamoto H, Shigematsu H, Suzuki S, Sakashita H. Regeneration of mandibular condyle following unilateral condylectomy in canines. J Craniomaxillofac Surg. 2004. 32:296–302.
Article12. Ferguson JW. Definitive surgical correction of the deformity resulting from hemimandibular hyperplasia. J Craniomaxillofac Surg. 2005. 33:150–157.
Article13. Dimitroulis G, Slavin J. The effects of unilateral discectomy and condylectomy on the contralateral intact rabbit craniomandibular joint. J Oral Maxillofac Surg. 2006. 64:1261–1266.
Article14. Unlü RE, Uysal AC, Alagöz MS, Tekin F, Sensöz O. An unusual complication of condylectomy: fracture of the temporal bone and intratemporal facial paralysis. J Craniofac Surg. 2005. 16:185–189.
Article15. Wolford LM, Mehra P, Reiche-Fischel O, Morales-Ryan CA, Garcia-Morales P. Efficacy of high condylectomy for management of condylar hyperplasia. Am J Orthod Dentofacial Orthop. 2002. 121:136–150.
Article16. Bertolini F, Bianchi B, De Riu G, Di Blasio A, Sesenna E. Hemimandibular hyperplasia treated by early high condylectomy: a case report. Int J Adult Orthodon Orthognath Surg. 2001. 16:227–234.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report Of Facial Asymmetry From Unilateral Condylar Hyperplasia
- Surgery-early approach combined with condylectomy for correction of severe facial asymmetry with mandibular condylar hyperplasia: a case report
- Conservative condylectomy alone for the correction of mandibular asymmetry caused by osteochondroma of the mandibular condyle: a report of five cases
- Assessment of functional improvement with temporalis myofascial flap after condylectomy in elderly patients with anterior disc displacement without reduction and an erosive condylar surface
- Condylar Hyperplasia with Long-standing Temporomandibular Joint Dislocation
