Long-term pharyngeal airway changes after bionator treatment in adolescents with skeletal Class II malocclusions
- Affiliations
-
- 1Department of Orthodontics, College of Dentistry, Yonsei University, Seoul, Korea. khkim@yuhs.ac
- 2Department of Orthodontics, Gangnam Severance Dental Hospital, Institute of Craniofacial Deformity, College of Dentistry, Yonsei University, Seoul, Korea.
- KMID: 2273266
- DOI: http://doi.org/10.4041/kjod.2014.44.1.13
Abstract
OBJECTIVE
The aim of this study was to evaluate long-term changes in the pharyngeal airway dimensions after functional appliance treatment in adolescents with skeletal Class II malocclusions.
METHODS
Pharyngeal airway dimensions were compared between subjects with skeletal Class II malocclusions (n = 24; mean age: 11.6 +/- 1.29 years) treated with a Class II bionator and age-matched control subjects with skeletal Class I occlusions (n = 24; mean age: 11.0 +/- 1.21 years) using a series of lateral cephalograms obtained at the initial visit (T0), after treatment (T1), and at the completion of growth (T2).
RESULTS
The length of the nasopharyngeal region was similar between adolescents with skeletal Class I and Class II malocclusions at all time points, while the lengths of the upper and lower oropharyngeal regions and the pharyngeal airway areas were significantly smaller in the skeletal Class II adolescents before treatment when compared to the control adolescents (p < 0.05). However, following treatment with a functional appliance, the skeletal Class II adolescents had increased pharyngeal airway dimensions, which became similar to those of the control subjects.
CONCLUSIONS
Functional appliance therapy can increase the pharyngeal airway dimensions in growing adolescents with skeletal Class II malocclusions, and this effect is maintained until the completion of growth.
Figure
-
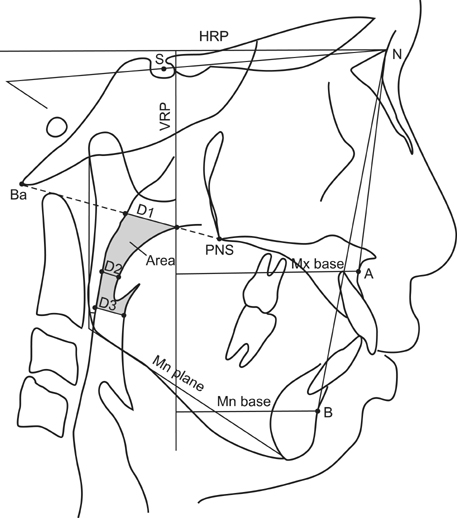
Figure 1 Measurements of linear, angular, and pharyngeal airway dimensions. HRP, horizontal reference plane; VRP, vertical reference plane; S, Sella; N, Nasion; Ba, Basion; PNS, posterior nasal spine; A, A point; B, B point; D1, the length at which the PNS-Ba line intersects the pharyngeal airway; D2, the narrowest distance between the soft palate and the posterior pharyngeal wall; D3, the narrowest distance between the base of tongue and the posterior pharyngeal wall; Area, the area between D1 and D3. Mx base and Mn base indicate A point and B point perpendicular distances to VRP, respectively. Mn plane indicates Gonion-Menton line.
Cited by 4 articles
-
Predictors of favorable soft tissue profile outcomes following Class II Twin-block treatment
Ji-Eun Kim, Su-Jung Mah, Tae-Woo Kim, Su-Jung Kim, Ki-Ho Park, Yoon-Goo Kang
Korean J Orthod. 2018;48(1):11-22. doi: 10.4041/kjod.2018.48.1.11.Pharyngeal airway dimensions in skeletal class II: A cephalometric growth study
Ozge Uslu-Akcam
Imaging Sci Dent. 2017;47(1):1-9. doi: 10.5624/isd.2017.47.1.1.Immediate effects of mandibular posterior displacement on the pharyngeal airway space: A preliminary study
Yeonju Choi, Yong-Il Kim, Seong-Sik Kim, Soo-Byung Park, Woo-Sung Son, Sung-Hun Kim
Korean J Orthod. 2020;50(2):129-135. doi: 10.4041/kjod.2020.50.2.129.Maxillomandibular advancement surgery after long-term use of a mandibular advancement device in a post-adolescent patient with obstructive sleep apnea
Keun-Ha Lee, Kyung-A Kim, Yong-Dae Kwon, Sung-Wan Kim, Su-Jung Kim
Korean J Orthod. 2019;49(4):265-276. doi: 10.4041/kjod.2019.49.4.265.
Reference
-
1. Li Y. Early orthodontic treatment of skeletal Class II malocclusion may be effective to prevent the potential for OSAHS and snoring. Med Hypotheses. 2009; 73:594–595.
Article2. Kim YJ, Hong JS, Hwang YI, Park YH. Three-dimensional analysis of pharyngeal airway in preadolescent children with different anteroposterior skeletal patterns. Am J Orthod Dentofacial Orthop. 2010; 137:306.e1–306.e11.
Article3. Subtelny JD. To treat or not to treat. Int Dent J. 1973; 23:292–303.4. Bishara SE, Hoppens BJ, Jakobsen JR, Kohout FJ. Changes in the molar relationship between the deciduous and permanent dentitions: a longitudinal study. Am J Orthod Dentofacial Orthop. 1988; 93:19–28.
Article5. You ZH, Fishman LS, Rosenblum RE, Subtelny JD. Dentoalveolar changes related to mandibular forward growth in untreated Class II persons. Am J Orthod Dentofacial Orthop. 2001; 120:598–607.
Article6. Proffit WR, Fields HW, Sarver DM. Contemporary orthodontics. 5th ed. St. Louis: Elsevier;2012. p. 141–145.7. Späth-Schwalbe E, Hundenborn C, Kern W, Fehm HL, Born J. Nocturnal wakefulness inhibits growth hormone (GH)-releasing hormone-induced GH secretion. J Clin Endocrinol Metab. 1995; 80:214–219.
Article8. Born J, Muth S, Fehm HL. The significance of sleep onset and slow wave sleep for nocturnal release of growth hormone (GH) and cortisol. Psychoneuroendocrinology. 1988; 13:233–243.
Article9. Agren K, Nordlander B, Linder-Aronsson S, Zettergren-Wijk L, Svanborg E. Children with nocturnal upper airway obstruction: postoperative orthodontic and respiratory improvement. Acta Otolaryngol. 1998; 118:581–587.
Article10. Williams EF 3rd, Woo P, Miller R, Kellman RM. The effects of adenotonsillectomy on growth in young children. Otolaryngol Head Neck Surg. 1991; 104:509–516.
Article11. Hiyama S, Kuribayashi G, Ono T, Ishiwata Y, Kuroda T. Nocturnal masseter and suprahyoid muscle activity induced by wearing a bionator. Angle Orthod. 2002; 72:48–54.12. Ozbek MM, Memikoglu TU, Gögen H, Lowe AA, Baspinar E. Oropharyngeal airway dimensions and functional-orthopedic treatment in skeletal Class II cases. Angle Orthod. 1998; 68:327–336.13. Hänggi MP, Teuscher UM, Roos M, Peltomäki TA. Long-term changes in pharyngeal airway dimensions following activator-headgear and fixed appliance treatment. Eur J Orthod. 2008; 30:598–605.
Article14. Fishman LS. Radiographic evaluation of skeletal maturation. A clinically oriented method based on hand-wrist films. Angle Orthod. 1982; 52:88–112.15. Baccetti T, Franchi L, McNamara JA Jr, Tollaro I. Early dentofacial features of Class II malocclusion: a longitudinal study from the deciduous through the mixed dentition. Am J Orthod Dentofacial Orthop. 1997; 111:502–509.
Article16. Goncalves JR, Buschang PH, Goncalves DG, Wolford LM. Postsurgical stability of oropharyngeal airway changes following counter-clockwise maxillo-mandibular advancement surgery. J Oral Maxillofac Surg. 2006; 64:755–762.
Article17. Restrepo C, Santamaría A, Peláez S, Tapias A. Oropharyngeal airway dimensions after treatment with functional appliances in class II retrognathic children. J Oral Rehabil. 2011; 38:588–594.
Article18. Hwang CJ, Ryu YK. A longitudinal study of nasopharynx and adenoid growth of Korean children. Korean J Orthod. 1985; 15:93–103.19. Harris JA, Jacksn CM, Paterson DG, Scammon RE. The measurement of man. Minneapolis: University of Minnesota Press;1930.20. Subtelny JD, Baker HK. The significance of adenoid tissue in velopharyngeal function. Plast Reconstr Surg (1946). 1956; 17:235–250.
Article21. Avrahami E, Englender M. Relation between CT axial cross-sectional area of the oropharynx and obstructive sleep apnea syndrome in adults. AJNR Am J Neuroradiol. 1995; 16:135–140.22. Abu Allhaija ES, Al-Khateeb SN. Uvulo-glosso-pharyngeal dimensions in different anteroposterior skeletal patterns. Angle Orthod. 2005; 75:1012–1018.23. Ceylan I, Oktay H. A study on the pharyngeal size in different skeletal patterns. Am J Orthod Dentofacial Orthop. 1995; 108:69–75.
Article24. Rose EC, Germann M, Sorichter S, Jonas IE. Case control study in the treatment of obstructive sleep-disordered breathing with an intraoral protrusive appliance. J Orofac Orthop. 2004; 65:489–500.
Article25. McNamara JA Jr. A method of cephalometric evaluation. Am J Orthod. 1984; 86:449–469.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pharyngeal Airway Dimensions in Skeletal Class II Young Adolescents : Cephalometric Study
- A study of the calcification of the second and the third molars in skeletal Class II and III malocclusions
- Does surgically assisted maxillary protraction with skeletal anchorage and Class III elastics affect the pharyngeal airway? A retrospective, long-term study
- An evaluation of treatment effects of bionator in Class II division 1 malocclusion by finite element method
- An evaluation of treatment effects of modified teuscher appliance in Class II division 1 malocclusion
