Ultrasound-Guided Lateral Femoral Cutaneous Nerve Conduction Study
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Korea University Guro Hospital, Seoul, Korea. snamyang@korea.ac.kr
- KMID: 2273018
- DOI: http://doi.org/10.5535/arm.2015.39.1.47
Abstract
OBJECTIVE
To verify the utility of the lateral femoral cutaneous nerve (LFCN) ultrasound-guided conduction technique compared to that of the conventional nerve conduction technique.
METHODS
Fifty-eight legs of 29 healthy participants (18 males and 11 females; mean age, 42.7+/-14.9 years) were recruited. The conventional technique was performed bilaterally. The LFCN was localized by ultrasound. Cross-sectional area (CSA) of the LFCN and the distance between the anterior superior iliac spine (ASIS) and the LFCN was measured. The nerve conduction study was repeated with the corrected cathode location. Sensory nerve action potential (SNAP) amplitudes of the LFCN were recorded and compared between the ultrasound-guided and conventional techniques.
RESULTS
Mean body mass index of the participants was 23.7+/-3.5 kg/m2, CSA was 4.2+/-1.9 mm2, and the distance between the ASIS and LFCN was 5.6+/-1.7 mm. The mean amplitude values were 6.07+/-0.52 microV and 6.66+/-0.54 microV using the conventional and ultrasound-guided techniques, respectively. The SNAP amplitude of the LFCN using the ultrasound-guided technique was significantly larger than that recorded using the conventional technique.
CONCLUSION
Correcting the stimulation position using the ultrasound-guided technique helped obtain increased SNAP amplitude.
Keyword
MeSH Terms
Figure
-

Fig. 1 The E1 electrode was placed 12 cm distal to the anterior superior iliac spine (ASIS) along an imaginary line between the ASIS and the lateral border of the patella. The E2 electrode was placed 4 cm distal to the E1. Stimulation was performed with a stimulator placed 1 cm medial to the ASIS.
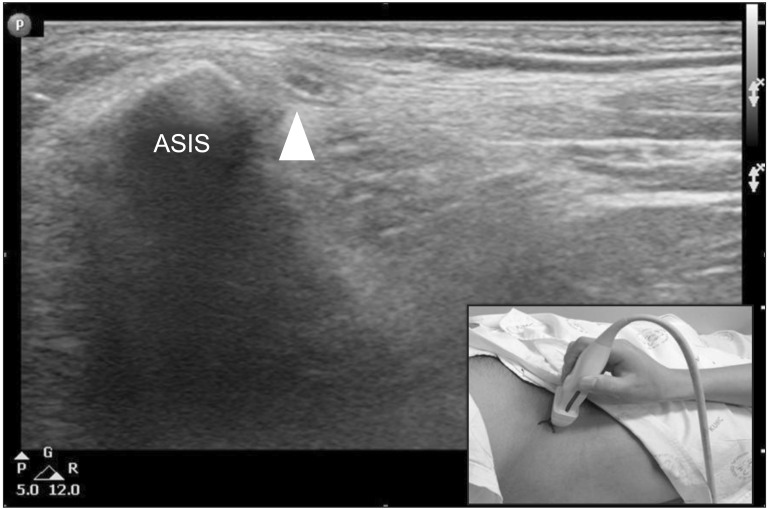
Fig. 2 Sonographic findings of the lateral femoral cutaneous nerve at the anterior superior iliac spine (ASIS) (arrowhead).

Fig. 3 (A) Photograph of the stimulation site for the lateral femoral cutaneous nerve conduction study using the conventional technique (arrow) and the ultrasound-guided technique (arrowhead) around the anterior superior iliac spine (ASIS) (asterisks). (B) Sensory nerve action potential (SNAP) of the lateral femoral cutaneous nerve (LFCN) using the conventional technique. (C) SNAP of the LFCN using the ultrasound-guided technique.
Cited by 2 articles
-
Optimal Radial Motor Nerve Conduction Study Using Ultrasound in Healthy Adults
Jungho Yeo, Yuntae Kim, Sooa Kim, Kiyoung Oh, Hyungdong Kang
Ann Rehabil Med. 2017;41(2):290-298. doi: 10.5535/arm.2017.41.2.290.Effect of Fascia Penetration in Lateral Femoral Cutaneous Nerve Conduction
Mi-Jeong Yoon, Hye Min Park, Sun Jae Won
Ann Rehabil Med. 2020;44(6):459-467. doi: 10.5535/arm.20022.
Reference
-
1. Patijn J, Mekhail N, Hayek S, Lataster A, van Kleef M, Van Zundert J. Meralgia paresthetica. Pain Pract. 2011; 11:302–308. PMID: 21435164.
Article2. Keegan JJ, Holyoke EA. Meralgia paresthetica. An anatomical and surgical study. J Neurosurg. 1962; 19:341–345. PMID: 14454774.3. Shin YB, Park JH, Kwon DR, Park BK. Variability in conduction of the lateral femoral cutaneous nerve. Muscle Nerve. 2006; 33:645–649. PMID: 16421869.
Article4. de Ridder VA, de Lange S, Popta JV. Anatomical variations of the lateral femoral cutaneous nerve and the consequences for surgery. J Orthop Trauma. 1999; 13:207–211. PMID: 10206253.
Article5. Kosiyatrakul A, Nuansalee N, Luenam S, Koonchornboon T, Prachaporn S. The anatomical variation of the lateral femoral cutaneous nerve in relation to the anterior superior iliac spine and the iliac crest. Musculoskelet Surg. 2010; 94:17–20. PMID: 20135245.
Article6. Aszmann OC, Dellon ES, Dellon AL. Anatomical course of the lateral femoral cutaneous nerve and its susceptibility to compression and injury. Plast Reconstr Surg. 1997; 100:600–604. PMID: 9283556.
Article7. Won SJ, Kim BJ, Park KS, Yoon JS, Choi H. Reference values for nerve ultrasonography in the upper extremity. Muscle Nerve. 2013; 47:864–871. PMID: 23625758.
Article8. Yang SN, Yoon JS, Kim SJ, Kang HJ, Kim SH. Movement of the ulnar nerve at the elbow: a sonographic study. J Ultrasound Med. 2013; 32:1747–1752. PMID: 24065255.9. Duncan I, Sullivan P, Lomas F. Sonography in the diagnosis of carpal tunnel syndrome. AJR Am J Roentgenol. 1999; 173:681–684. PMID: 10470903.
Article10. Suh DH, Kim DH, Park JW, Park BK. Sonographic and electrophysiologic findings in patients with meralgia paresthetica. Clin Neurophysiol. 2013; 124:1460–1464. PMID: 23474056.
Article11. Zhu J, Zhao Y, Liu F, Huang Y, Shao J, Hu B. Ultrasound of the lateral femoral cutaneous nerve in asymptomatic adults. BMC Musculoskelet Disord. 2012; 13:227. PMID: 23171132.
Article12. Damarey B, Demondion X, Boutry N, Kim HJ, Wavreille G, Cotten A. Sonographic assessment of the lateral femoral cutaneous nerve. J Clin Ultrasound. 2009; 37:89–95. PMID: 18803312.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasound-guided Nerve Block for Skin Grafting on Large Diabetic Ulcer of Foot and Leg: A Technical Report
- The Efficacy of Ultrasound-Guided Lower Extremity Nerve Block in Trauma Patients
- Ultrasound-guided Lateral Femoral Cutaneous Nerve Block in Meralgia Paresthetica
- Ultrasound-Guided Pain Interventions: A Review of Techniques for Peripheral Nerves
- Lateral Femoral Cutaneous Nerve Conduction Study
