Ruptured Popliteal Cyst Diagnosed by Ultrasound Before Evaluation for Deep Vein Thrombosis
- Affiliations
-
- 1Department of Rehabilitation Medicine, The Catholic University of Korea College of Medicine, Seoul, Korea. lsh728@naver.com
- KMID: 2267096
- DOI: http://doi.org/10.5535/arm.2014.38.6.843
Abstract
- Most popliteal cysts are asymptomatic. However, cysts may rupture, resulting in pain and swelling of the leg that could also arise from other diseases, including deep vein thrombosis, lymphedema, cellulitis, and tear of a muscle or tendon. Therefore, it is difficult to diagnose a ruptured popliteal cyst based on only a patient's history and physical examination. Musculoskeletal ultrasound has been regarded as a diagnostic tool for ruptured popliteal cyst. Here, we describe a patient who was rapidly diagnosed as ruptured popliteal cyst by ultrasonography. Therefore, ultrasound could be used to distinguish a ruptured popliteal cyst from other diseases in patients with painful swollen legs before evaluation for deep vein thrombosis.
MeSH Terms
Figure
-

Fig. 1 Physical examination of unilateral leg swelling accompanied by slight redness and warmth was noted in the patient's left leg.
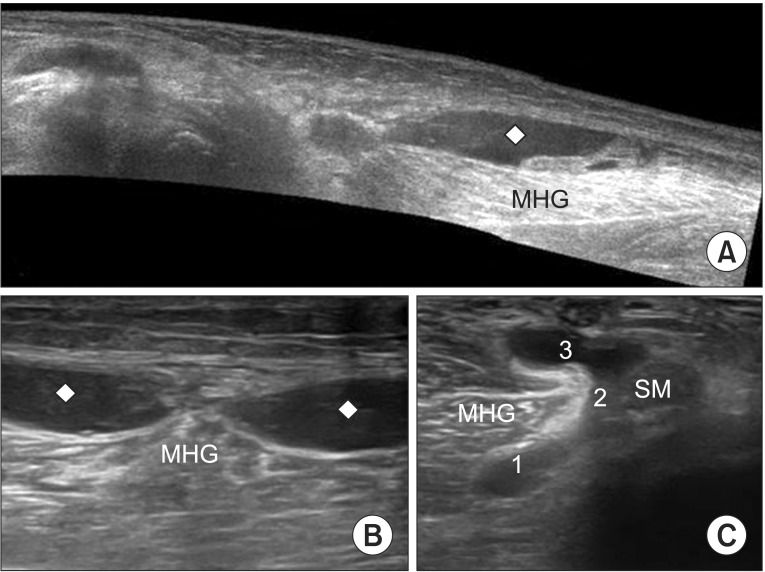
Fig. 2 Ultrasonography images. (A) Panoramic image of the longitudinal sweep of the medial aspect of calf shows fluid collection (rhomboid) behind medial head of the gastrocnemius muscle (MHG). (B) Transverse 12-5 MHz ultrasound image over the proximal medial calf shows the fluid collection separated into two compartments. (C) Transverse 12-5 MHz ultrasound image over the popliteal fossa shows the different components of a typical popliteal cyst: the base '1', the neck '2', and the body '3' located between the tendon of the semimembranosus (SM) and the tendon of the MHG.

Fig. 3 Initially a 10 mL of dark red-colored liquid was drained from the calf.
Reference
-
1. Ward EE, Jacobson JA, Fessell DP, Hayes CW, van Holsbeeck M. Sonographic detection of Baker's cysts: comparison with MR imaging. AJR Am J Roentgenol. 2001; 176:373–380. PMID: 11159077.2. Dunlop D, Parker PJ, Keating JF. Ruptured Baker's cyst causing posterior compartment syndrome. Injury. 1997; 28:561–562. PMID: 9616400.
Article3. Sato O, Kondoh K, Iyori K, Kimura H. Midcalf ultrasonography for the diagnosis of ruptured Baker's cysts. Surg Today. 2001; 31:410–413. PMID: 11381504.
Article4. Kane D, Balint PV, Gibney R, Bresnihan B, Sturrock RD. Differential diagnosis of calf pain with musculoskeletal ultrasound imaging. Ann Rheum Dis. 2004; 63:11–14. PMID: 14672884.
Article5. Liao ST, Chiou CS, Chang CC. Pathology associated to the Baker's cysts: a musculoskeletal ultrasound study. Clin Rheumatol. 2010; 29:1043–1047. PMID: 20535511.
Article6. Molla Olmos E, Marti-Bonmati L, Llombart Ais R, Dosda Munoz R. Prevalence and characteristics of complications of Baker cysts by MRI. Rev Clin Esp. 2001; 201:179–183. PMID: 11447901.7. Romem A, Shimony A, Horowitz S, Horowitz J. Popliteal cyst rupture due to unusual physical stress. Harefuah. 2007; 146:653–654. 736PMID: 17969298.8. Volteas SK, Labropoulos N, Leon M, Kalodiki E, Nicolaides AN. Incidence of ruptured Baker's cyst among patients with symptoms of deep vein thrombosis. Br J Surg. 1997; 84:342. PMID: 9117303.
Article9. Klovning J, Beadle T. Compartment syndrome secondary to spontaneous rupture of a Baker's cyst. J La State Med Soc. 2007; 159:43–44. PMID: 17396475.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ruptured Popliteal Cyst in Gouty Arthritis
- A Popliteal Cyst Causing Tibial Nerve Entrapment Neuropathy: A Case Report
- Popliteal Artery Aneurysm Presenting as Acute Deep Vein Thrombosis
- Arterivenous Fistula Complicated by Popliteal Venous Access for Endovascular Thrombolytic Therapy of Deep Vein Thrombosis
- Adventitial Cystic Disease of the Common Femoral Vein Mimicking Deep Venous Thrombosis: A Case Report
