Ann Rehabil Med.
2011 Dec;35(6):954-957. 10.5535/arm.2011.35.6.954.
A Nasogastric Tube Inserted into the Gastrocutaneous Fistula
- Affiliations
-
- 1Department of Rehabilitation Medicine, College of Medicine, The Catholic University of Korea, Seoul 130-709, Korea. coltrane@catholic.ac.kr
- KMID: 2266825
- DOI: http://doi.org/10.5535/arm.2011.35.6.954
Abstract
- We reported a case in which a nasogastric tube was inserted into the gastrocutaneous fistula, diagnosed by abdominal computed tomography. A 78-year-old man with a history of recurrent cerebral hemorrhage had a percutaneous endoscopic gastrostomy tube due to dysphagia for 2 years. However, soft tissue infection at the gastrostomy site caused the removal of the tube. Immediately, antibiotic agents were infused. For appropriate hydration and medication, a nasogastric tube was inserted. However, there was no significant improvement of the soft tissue infection. Moreover, the amount of bloody exudate increased. Abdominal computed tomography revealed the nasogastric tube placed under the patient's skin via gastrocutaneous fistula. The nasogastric tube was removed, and an antibiotic agents were maintained. After 3 weeks, the signs of infection fully improved, and percutaneous endoscopic gastrostomy was performed again. This case shows necessities of an appropriate interval between removal of the gastrostomy tube and insertion of a nasogastric tube, and suspicion of existence of gastrocutaneous fistula.
MeSH Terms
Figure
-
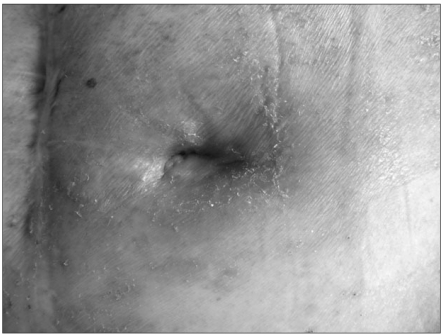
Fig. 1 Erythematous skin is observed in the gastrostomy site after removal of tube.
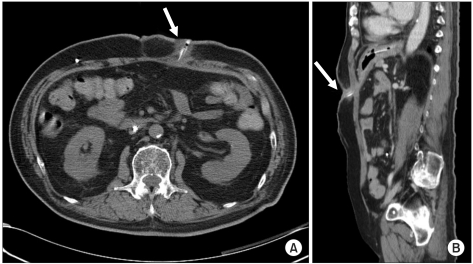
Fig. 2 CT findings show a transverse cut (A) and a coronal cut (B) of nasogastric tube placed beneath the skin via gastrocutaneous fistula.
Reference
-
1. Veis SL, Longemann JA. Swallowing disorders in persons with cerebrovascular accident. Arch Phys Med Rehabil. 1985; 66:372–375. PMID: 4004534.2. Penington GR, Krutsch JA. Swallowing disorders: assessment and rehabilitation. Br J Hosp Med. 1990; 44:17–22. PMID: 2118817.3. Raha SK, Woodhouse KW. Who should have a PEG? Age Ageing. 1993; 22:313–315. PMID: 8237619.
Article4. Pien EC, Hume KE, Pien FD. Gastrostomy tube infections in a community hospital. Am J Infect Control. 1996; 24:353–358. PMID: 8902109.
Article5. Wynne DM, Borg HK, Geddes NK, Fredericks B. Nasogastric tube misplacement into Eustachian tube. Int J Pediatr Otorhinolaryngol. 2003; 67:185–187. PMID: 12623157.
Article6. Sorokin R, Gottlieb JE. Enhancing patient safety during feeding-tube insertion: a review of more than 2000 insertions. JPEN J Parenter Enteral Nutr. 2006; 30:440–445. PMID: 16931614.
Article7. Rahimi-Movaghar V, Boroojeny SB, Moghtaderi A, Keshimirian B. Intracranial placement of a nasogastric tube. A lesson to be re-learnt? Acta Neurochir (Wien). 2005; 147:573–574. PMID: 15625586.
Article8. Aronian JM, Redo SF. Gastrocutaneous fistula after tube gastrostomy. Incidence in infants and children. N Y State J Med. 1974; 74:2364–2366. PMID: 4530926.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Successful management of a chronic post-surgical gastrocutaneous fistula using as a route for enteral feeding tube placement: A case report
- Conversion of Percutaneous Endoscopic Gastrostomy to Gastrojejunostomy Under Fluoroscopic Guidance for Treatment of Gastrocutaneous Fistula
- The Insertion of a Nasogastric Tube with a Nasopharyngeal Airway
- A study on The Applying of Training Program to Facilitate Deglution: On spontaneous intracerebral hemorrhage patients with nasogastric tube
- Repair of Tracheoesophageal Fistula under Laryngeal Microsurgery Approach: Case Report and Literature Review
