An Objective Assessment Scale for "Come-to-Sit" Using a Specifically Designed Jacket in Stroke Patients
- Affiliations
-
- 1Department of Physical & Rehabilitation Medicine, Inha University School of Medicine, Incheon 400-711, Korea. rmkmo@inha.ac.kr
- 2Department of Physics, Inha University, Incheon 400-711, Korea.
- 3Technical Aid Center, Notre-dame Welfare Center, Incheon 400-711, Korea.
- KMID: 2266775
- DOI: http://doi.org/10.5535/arm.2012.36.1.8
Abstract
OBJECTIVE
To compare an objective assessment scale for "come-to-sit" in stroke patients with the previously established subjective assessment scales of "performance-based assessment" and the "ability for basic movement scale". METHOD: A specifically designed jacket was used to determine the objective degree of assistance needed for patients to perform the task. While patients were sitting up, the investigator evaluated the amount of assistance needed in a fully dependent state (A) and with maximal effort (B). Using this measure, we obtained an objective scale, {(A-B)/A} x100. In addition, patients were tested in two starting positions: hemiplegic-side lying and sound-side lying. We then compared the objective scale with subjective scales and other parameters related to functional outcomes.
RESULTS
For both starting positions, the objective assessment scale showed high correlation with the previously established subjective scales (p<0.01). Only the hemiplegic-side lying-to-sit objective scale showed a significant correlation with the parameters used to assess functional outcomes (p<0.05). In terms of Brunnstrom stages, only the leg stage showed a significant correlation with the objective "come-to-sit" scale (p<0.01).
CONCLUSION
The objective scale was comparable to established subjective assessment scales when used by an expert. The hemiplegic-side lying-to-sit maneuver had a high correlation with patient's functional recovery. Specifically, balance and lower extremity function appear to be important factors in the "come-to-sit" activity.
Figure
-
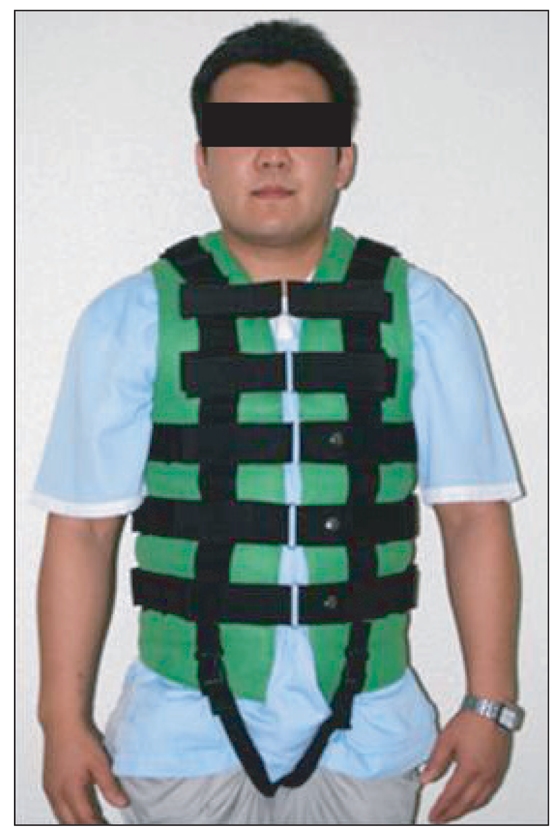
Fig. 1 The specifically designed jacket was applied to pull the patient's trunk so as to measure the weight.

Fig. 2 Scale measuring the maximal value of pulling weight (Travelon®, Elk Grove Village, USA).
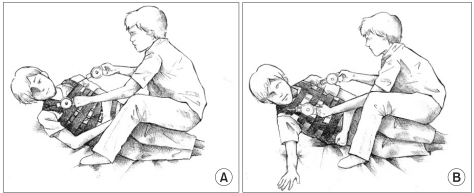
Fig. 3 (A) Total assisted sitting with full dependence. (B) Active assisted sitting with full effort.
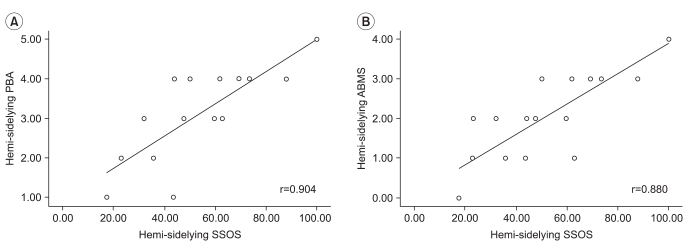
Fig. 4 (A) The correlations between SSOS and PBA at the hemiplegic side. (B) The correlations between SSOS and ABMS at the hemiplegic side. SSOS: Side lying to sit objective scale, PBA: Performance-based assessment, ABMS: The ability for basic movement scale.
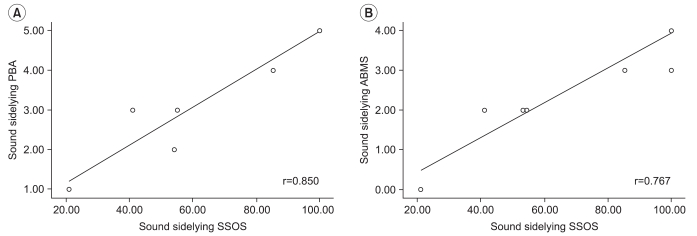
Fig. 5 (A) The correlations between SSOS and PBA at the sound side. (B) The correlations between SSOS and ABMS at the sound side. SSOS: Side lying to sit objective scale, PBA: Performance-based assessment, ABMS: The ability for basic movement scale.
Reference
-
1. Chon JS, Chun SI, Kim DA, Seo CH, Yun TJ, Jang YW. The analysis of sit-to-stand motion in stroke patient. J Korean Acad Rehabil Med. 2000; 24:850–856.2. Kim MG, Kim SH, Yang SH, Son SG. An analysis of the movements during rising from a chair. J Korean Acad Rehabil Med. 1995; 19:23–31.3. Hsieh CL, Sheu CF, Hsueh IP, Wang CH. Trunk control as an early predictor of comprehensive activities of daily living function in stroke patients. Stroke. 2002; 33:2626–2630. PMID: 12411652.
Article4. Susan RY, Kathryn LE. Functional movement reeducation. 1997. 1st ed. New York: Churchill Livingstone;p. 375–396.5. Susan BO. Physical rehabilitation assessment and treatment. 1994. 3rd ed. Philadelphia: F.A. Davis Company;p. 196–197.6. Hashimoto K, Hiquchi K, Nakayama Y, Abo M. Ability for basic movement as an early predictor of functioning related to activities of daily living in stroke patients. Neurorehabil Neural Repair. 2007; 21:353–357. PMID: 17369512.
Article7. Jung HY, Park JH, Shim JJ, Kim MJ, Hwang MR, Kim SH. Reliability test of Korean version of berg balance scale. J Korean Acad Rehabil Med. 2006; 30:611–618.8. Jung HY, Park BK, Shin HS, Kang YK, Pyun SB, Nam JP, Kim SH, Kim TH, Han TR. Development of the Korean version of modified barthel index (K-MBI): multicenter study for subjects with stroke. J Korean Acad Rehabil Med. 2007; 31:283–297.9. Jhoo JH, Kim KW, Lee DY, Youn JC, Lee TJ, Choo IH, Ko HJ, Seo EH, Woo JI. Comparison of the performance in two different Korean versions of minimental status examination: MMSE-KC and K-MMSE. J Korean Neuropsychiatr Assoc. 2005; 44:98–104.10. Brandstater ME. Delisa JA, editor. Stroke rehabilitation. Physical medicine and rehabilitation. 2005. 4th ed. Philadelpia: Lippincott Williams & Wilkins;p. 1667–1668.11. Molnar GE, Gordon SU. Cerebral palsy: predictive value of selected clinical signs of early prognostication of motor function. Arch Phys Med Rehabil. 1976; 57:153–158. PMID: 1267590.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biomechanical Analysis of Sit-to-stand Transfer in Stroke Patients: Comparison between Stable and Labile Surfaces
- The Effect of Treadmill Aerobic Exercise in Stroke Patients
- The Korean Version of Berg Balance Scale as an Index of Activity Related to Ambulation in Subjects with Stroke
- Factors Affecting Activities of Daily Living in Severely Disabled Stroke Patients
- The Analysis of Sit-to-Stand Motion in Stroke Patients
