Optimal Stimulation Site for Deep Peroneal Motor Nerve Conduction Study Around the Ankle: Cadaveric Study
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, College of Medicine, Korea University, Ansan 425-707, Korea. rmkdh@korea.ac.kr
- KMID: 2266755
- DOI: http://doi.org/10.5535/arm.2012.36.2.182
Abstract
OBJECTIVE
To identify the optimal distal stimulation point for conventional deep peroneal motor nerve (DPN) conduction studies by a cadaveric dissection study. METHOD: DPN was examined in 30 ankles from 20 cadavers. The distance from the DPN to the tibialis anterior (TA) tendon was estimated at a point 8 cm proximal to the extensor digitorum brevis (EDB) muscle. Relationships between the DPN and tendons including TA, extensor hallucis longus (EHL), and extensor digitorum longus (EDL) tendons were established.
RESULTS
The median distance from the DPN to the TA tendon in all 30 cadaver ankles was 10 mm (range, 1-21 mm) at a point 8 cm proximal to the EDB muscle. The DPN was situated between EHL and EDL tendons in 18 cases (60%), between TA and EHL tendons in nine cases (30%), and lateral to the EDL tendon in three cases (10%).
CONCLUSION
The optimal distal stimulation point for the DPN conduction study was approximately 1 cm lateral to the TA tendon at the level of 8 cm proximal to the active electrode. The distal stimulation site for the DPN should be reconsidered in cases with a weaker distal response but without an accessory peroneal nerve.
Keyword
Figure
-
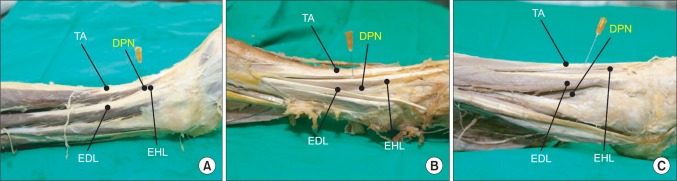
Fig. 1 Variation in the location of the deep peroneal nerve (DPN) at the ankle. (A) Type 1, in which the DPN is located between the tibialis anterior (TA) and extensor hallucis longus (EHL) tendons. (B) Type 2, in which the DPN is located between the EHL and extensor digitorum longus (EDL) tendons. (C) Type 3, in which the DPN is located lateral to the EDL tendon. Needle indicates just the lateral side of TA tendon at a point 8 cm proximal to the EDB muscle (DPN_TA).
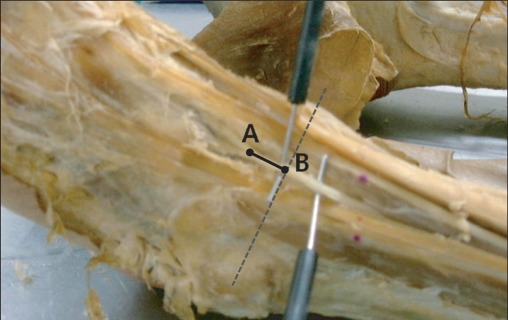
Fig. 2 The distance (DPN_CP) between the bifurcation (A) of the deep peroneal nerve (DPN) at the ankle and the point (B) at which the DPN crosses the mediolateral malleolar line (CP).
Cited by 1 articles
-
Optimal Needle Placement for Extensor Hallucis Longus Muscle: A Cadaveric Study
In Yae Cheong, Do Kyun Kim, Ye Jeong Oh, Byung Kyu Park, Ki Hoon Kim, Dong Hwee Kim
Ann Rehabil Med. 2016;40(3):457-462. doi: 10.5535/arm.2016.40.3.457.
Reference
-
1. Dumitru D, Amato AA, Zwarts M. Dumitru D, Amato AA, Zwarts M, editors. Nerve conduction studies. Electrodiagnostic medicine. 2002. 2nd ed. Philadelphia: Hanley & Belfus Inc.;p. 159–223.
Article2. Lee HJ, DeLisa JA. Manual of nerve conduction study and surface anatomy for needle electromyography. 2005. 4th ed. Philadelphia: Lippincott William & Wilkins;p. 67–71.3. Lambert EH. The accessory deep peroneal nerve. A common variation in innervation of extensor digitorum brevis. Neurology. 1969; 19:1169–1176. PMID: 5389696.
Article4. Neundorfer B, Seiberth R. The accessory deep peroneal nerve. J Neurol. 1975; 209:125–129. PMID: 51049.5. Stamboulis E. Accessory deep peroneal nerve. Electromyogr Clin Neurophysiol. 1987; 27:289–292. PMID: 3665814.6. Kim KH, Kim DH, Kang YK, Hwang MR, Shin JY. Optimal distal stimulation site in the peroneal motor nerve conduction study. J Korean Assoc EMG-Electrodiagn Med. 2003; 5:11–14.7. Horwitz MT. Normal anatomy and variations of the peripheral nerves of the leg and foot. Arch Surg. 1938; 36:626–636.
Article8. Lawrence SJ, Botte MJ. The deep peroneal nerve in the foot and ankle: an anatomic study. Foot Ankle Int. 1995; 16:724–728. PMID: 8589813.
Article9. Takao M, Uchio Y, Shu N, Ochi M. Anatomic bases of ankle arthoscopy: study of superficial and deep peroneal nerves around anterolateral and anterocentral approach. Surg Radiol Anat. 1998; 20:317–320. PMID: 9894310.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The accessory deep peroneal nerve : frequency and electrophysiological findings
- The Diagnostic Value of Segmental Nerve Conduction Study in Diabetics
- Electrophysiologic Study of Accessory Deep Peroneal Nerve
- Compression Neuropathy of Superficial Peroneal Nerve and Deep Peroneal Nerve Following Acupuncture Treatment: A Case Report
- Motor Nerve Conduction Velocity in Newborn Infants and Children
