Ann Rehabil Med.
2014 Oct;38(5):707-711. 10.5535/arm.2014.38.5.707.
Usefulness of Videofluoroscopic Swallow Study in Treacher Collins Syndrome With Cleft Palate: A Case Report
- Affiliations
-
- 1Department of Physical Medicine & Rehabilitation, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea. rehabkjh@hanmail.net
- 2Department of Pediatrics, Eulji University Hospital, Eulji University School of Medicine, Daejeon, Korea.
- KMID: 2266508
- DOI: http://doi.org/10.5535/arm.2014.38.5.707
Abstract
- A 3-year-old girl had multiple anomalies compatible with Treacher Collins Syndrome (TCS). From the neonatal period, sucking was poor, making tube feeding necessary. Excessive saliva was retained in the oral cavity. Nasal leakage caused by the cleft palate was observed when she spoke. The initial videofluoroscopic swallow study (VFSS) showed a poor posterior bolus transit and nasopharyngeal regurgitation. A delayed swallow reflex and bolus stasis at the vallecular and pyriform sinuses were recognized. Based on the VFSS findings, the patient underwent palatoplasty at 20 months of age. At approximately 23 months of age, a follow-up VFSS was performed; poor posterior bolus transit, nasopharyngeal regurgitation, and delayed swallow reflex were not observed. Finally, the patient was able to eat ground or chopped foods and solid foods orally. We deem VFSS to be helpful in deciding the appropriate management of dysphagia in TCS.
Keyword
MeSH Terms
Figure
-
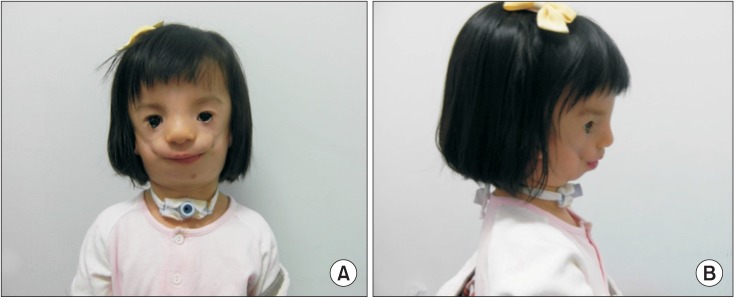
Fig. 1 Clinical features of the patient with facial abnormalities of Treacher Collins syndrome in the frontal (A) and lateral views (B).
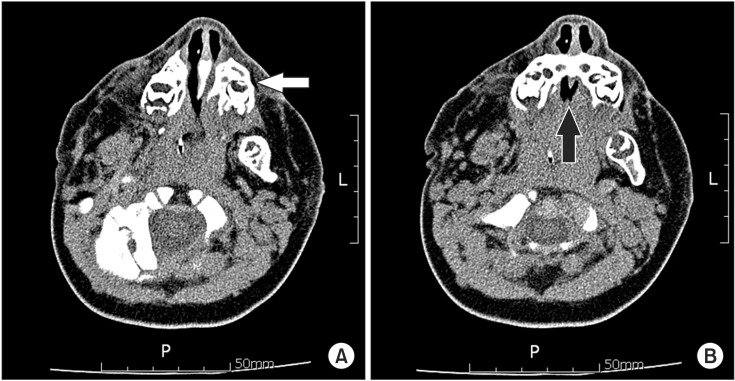
Fig. 2 Axial views of facial computed tomography show (A) hypoplasia of the maxilla (white arrow) and (B) hard palate defect (black arrow).
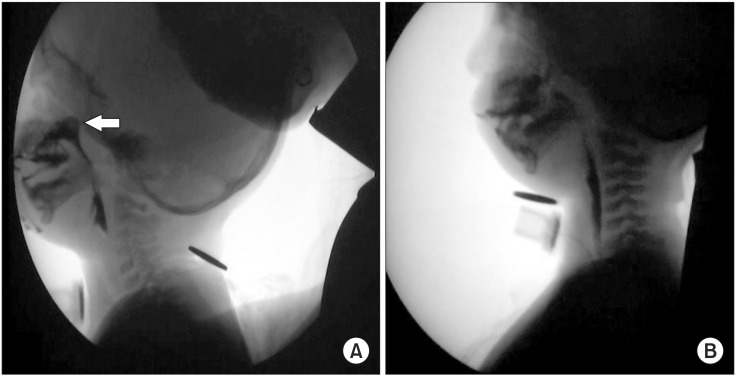
Fig. 3 (A) The first videofluoroscopic swallow study (VFSS) performed before surgical treatment shows nasopharyngeal regurgitation (white arrow) of a large amount of liquid during swallowing and (B) the second VFSS performed after surgical treatment do not show any evidence of nasopharyngeal regurgitation.
Reference
-
1. Posnick JC, Ruiz RL. Treacher Collins syndrome: current evaluation, treatment, and future directions. Cleft Palate Craniofac J. 2000; 37:434. PMID: 11034023.
Article3. Yokochi K, Terasawa S, Kono C, Fujishima I. Dysphagia in children with oculo-auriculo-vertebral spectrum. Dysphagia. 1997; 12:222–225. PMID: 9294943.
Article4. Logemann JA. Manual for the videofluorographic study of swallowing. 2nd ed. Austin, TX: Pro-Ed;1993.5. Hiorns MP, Ryan MM. Current practice in paediatric videofluoroscopy. Pediatr Radiol. 2006; 36:911–919. PMID: 16552584.
Article6. Liau JY, Sadove AM, van Aalst JA. An evidence-based approach to cleft palate repair. Plast Reconstr Surg. 2010; 126:2216–2221. PMID: 21124164.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Acute airway obstruction in an infant with treacher collins syndrome: Report of a case
- Fiberoptic Bronchoscopic Intubation in a Patient with Treacher-Collins Syndrome
- Management of obstructive sleep apnea in a Treacher Collins syndrome patient using distraction osteogenesis of the mandible
- Contouring of zygomatic soft tissue using bilateral free groin flaps in a Treacher Collins syndrome patient
- Airway management in a patient with Treacher Collins syndrome: A case report
