Current status of gynecologic cancer in Japan
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Kurume University School of Medicine, Kurume, Japan. kimi@med.kurume-u.ac.jp
- KMID: 2245082
- DOI: http://doi.org/10.3802/jgo.2009.20.2.67
Abstract
- To make an overview of the current status of gynecologic cancer in Japan, we reviewed the recent incidence of cervical, endometrial, and ovarian cancer in Japanese women. The incidence of all three cancers has increased, but trends differ respectively. In age specific cancer site distribution data, the uterus and ovary are leading sites of high incidence among Japanese women younger than 40 years of age. Therefore, fertility sparing cancer treatment has received much attention. Several multicenter clinical trials have been done by Japanese groups, and some excellent evidence has been collected for endometrial and ovarian cancer. A promising international collaboration trial for ovarian clear cell carcinoma is also underway at the present time.
Keyword
MeSH Terms
Figure
-

Fig. 1 Changes in site distribution of the cancer mortality rate of Japanese women. Uterine cancer decreased until 1995, then slightly increased. Ovarian cancer increased similar to breast, rectal and colon cancer.

Fig. 2 Changes in the age-specific incidence rate of cervical cancer in Japanese women. The total number of incidences decreased remarkably between 1980 and 2000. Nevertheless, there was an obvious elevation in the incidence rate for women in their 20's and 30's in 2000 (Source: center for cancer control and information services, National Cancer Center, Japan).

Fig. 3 Changes in the age-specific incidence rate of endometrial cancer. Total number of incidences obviously increased. The rise in younger patients stands out (Source: center for cancer control and information services, National Cancer Center, Japan).

Fig. 4 Changes in the age-specific incidence rate of ovarian cancer. A striking increase is shown in women at over sixty of age (Source: center for cancer control and information services, National Cancer Center, Japan).
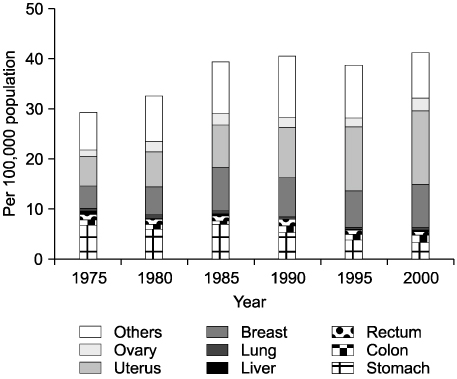
Fig. 5 Changes in site distribution of the cancer incidence rate for ages 0 to 39. The incidence of cancer in the female genital tract certainly has increased more than any other cancer site among younger women (Source: center for cancer control and information services, National Cancer Center, Japan).
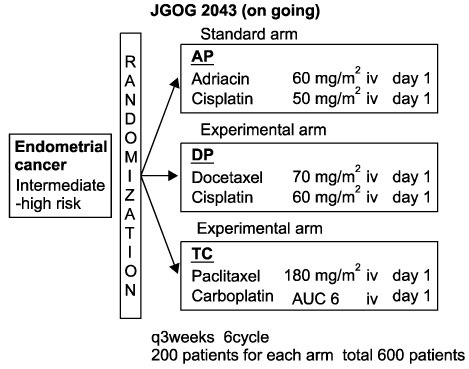
Fig. 6 Protocol scheme of JGOG 2043 for adjuvant chemotherapy for endometrial cancer. Patients eligibility: Patients who received surgical staging laparotomy, and pathologically confirmed endometrial cancer under the following conditions. 1) FIGO stage Ic to II, with grade 2 or 3 tumor (G3 included serous, clear, undifferentiated tumor). 2) FIGO stage III and IV tumor without distant metastasis. 3) age 20 to 75 years old, performance status 0-2, reasonable organ function.

Fig. 7 Protocol scheme of GCIG/JGOG 3017 for adjuvant chemotherapy for ovarian clear cell carcinoma patients eligibility: Patients with a pathologically confirmed clear cell carcinoma of the ovary. The histological diagnosis will be confirmed by central pathological review. Ages 18 or older, reasonable organ function. PFS: progression-free survival, OS: overall survival
Cited by 2 articles
-
Assessing the effect of guideline introduction on clinical practice and outcome in patients with endometrial cancer in Japan: a project of the Japan Society of Gynecologic Oncology (JSGO) guideline evaluation committee
Shogo Shigeta, Satoru Nagase, Mikio Mikami, Masae Ikeda, Masako Shida, Isao Sakaguchi, Norichika Ushioda, Fumiaki Takahashi, Wataru Yamagami, Nobuo Yaegashi, Yasuhiro Udagawa, Hidetaka Katabuchi
J Gynecol Oncol. 2017;28(6):e76. doi: 10.3802/jgo.2017.28.e76.Assessing the effect of guideline introduction on clinical practice and outcome in patients with endometrial cancer in Japan: a project of the Japan Society of Gynecologic Oncology (JSGO) guideline evaluation committee
Shogo Shigeta, Satoru Nagase, Mikio Mikami, Masae Ikeda, Masako Shida, Isao Sakaguchi, Norichika Ushioda, Fumiaki Takahashi, Wataru Yamagami, Nobuo Yaegashi, Yasuhiro Udagawa, Hidetaka Katabuchi
J Gynecol Oncol. 2017;28(6):. doi: 10.3802/jgo.2017.28.e76.
Reference
-
1. Oshima A, Kuroisi T, Tajima K. Cancer statistic statement. 2004. Tokyo: Shinohara Publishing.2. Report from gynecologic tumor committee of JSOG. Acta Obstet Gynaecol Jpn. 2007. 59:952.3. Report from gynecologic tumor committee of JSOG. Acta Obstet Gynaecol Jpn. 2009. 61:936.4. Report from gynecologic tumor committee of JSOG. Acta Obstet Gynaecol Jpn. 2000. 52:855.5. Kaku T, Yoshikawa H, Tsuda H, Sakamoto A, Fukunaga M, Kamura T, et al. Conservative therapy for adenocarcinoma and atypical endometrial hyperplasia of the endometrium in young women: central pathologic review and treatment outcome. Cancer Lett. 2001. 167:39–48.6. Ushijima K, Yahata H, Yoshikawa H, Konishi I, Yasugi T, Saito T, et al. Multicenter phase II study of fertility-sparing treatment with medroxyprogesterone acetate for endometrial carcinoma and atypical hyperplasia in young women. J Clin Oncol. 2007. 25:2798–2803.7. Japan Society of Gynecologic Oncology. Ovarian cancer treatment guidelines 2007. 2007. Tokyo: Kanehara & Co. Ltd.8. Susumu N, Sagae S, Udagawa Y, Niwa K, Kuramoto H, Satoh S, et al. Randomized phase III trial of pelvic radiotherapy versus cisplatin-based combined chemotherapy in patients with intermediate- and high-risk endometrial cancer: a Japanese Gynecologic Oncology Group study. Gynecol Oncol. 2008. 108:226–233.9. Rose PG, Smrekar M, Fusco N. A phase II trial of weekly paclitaxel and every 3 weeks of carboplatin in potentially platinum-sensitive ovarian and peritoneal carcinoma. Gynecol Oncol. 2005. 96:296–300.10. Isonishi S, Yasuda M, Takahashi F, Katsumata N, Kimura E, Aoki D, et al. Randomized phase III trial of conventional paclitaxel and carboplatin (c-TC) versus dose dense weekly paclitaxel and carboplatin (dd-TC) in women with advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer: Japanese Gynecologic Oncology [abstract]. J Clin Oncol. 2008. 26(15S):abstr 5506.11. Taguchi K. Clinical characteristics of clear cell carcinoma of the ovary: a distinct histologic type with poor prognosis and resistance to platinum-based chemotherapy. Cancer. 2000. 88:2584–2589.12. Enomoto T, Kuragaki C, Yamasaki M, Sugita N, Otsuki Y, Ikegami H, et al. Is clear cell carcinoma and mucinous carcinoma of the ovary sensitive to combination chemotherapy with paclitaxel and carboplatin? [abstract]. Proc Am Soc Clin Oncol. 2003. 22:abstr 1797.13. Sugiyama T, Yakushiji M, Nishida T, Ushijima K, Okura N, Kigawa J, et al. Irinotecan (CPT-11) combined with cisplatin in patients with refractory or recurrent ovarian cancer. Cancer Lett. 1998. 128:211–218.14. Takano M, Kikuchi Y, Yaegashi N, Suzuki M, Tsuda H, Sagae S, et al. Adjuvant chemotherapy with irinotecan hydrochloride and cisplatin for clear cell carcinoma of the ovary. Oncol Rep. 2006. 16:1301–1306.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current status and future directions of ovarian cancer prognostic models
- Annual report of gynecologic cancer registry program in Korea: 1991~2004
- Towards the elimination of cervical cancer in Japan
- Current status of hereditary breast and ovarian cancer practice among gynecologic oncologists in Japan: a nationwide survey by the Japan Society of Gynecologic Oncology (JSGO)
- The current status of laparoscopic and robotic para-aortic lymphadenectomy in gynecologic cancer surgery
