Spontaneous rupture of intrahepatic bile duct following portal vein embolization in a patient with perihilar cholangiocarcinoma: a case of successful curative resection
- Affiliations
-
- 1Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. shwang@amc.seoul.kr
- 2Department of Diagnostic Radiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2243169
- DOI: http://doi.org/10.14701/kjhbps.2013.17.1.42
Abstract
- We herein present a case of spontaneous rupture of intrahepatic bile duct in a patient with perihilar cholangiocarcinoma, which were successfully treated by curative resection. A 60-year-old male patient with perihilar cholangiocarcinoma was decompressed with single percutaneous transhepatic biliary drainage. Two days after right portal vein embolization, the patient suffered from paralytic ileus with marked abdominal distension. Imaging study revealed that marked fluid collection around the liver and whole abdomen, suggesting intrahepatic bile duct rupture. With abdominal drainage and biliary decompression for 2 weeks, the biliary rupture was controlled. To enhance the safety of right hepatectomy, additional right hepatic vein embolization was performed. The patient underwent routine surgical procedures for right hepatectomy, caudate lobectomy and bile duct resection, and recovered uneventfully and discharged 18 days after surgery. This is the first report of a case of spontaneous rupture of intrahepatic bile duct in a patient with perihilar cholangiocarcinoma.
MeSH Terms
Figure
-
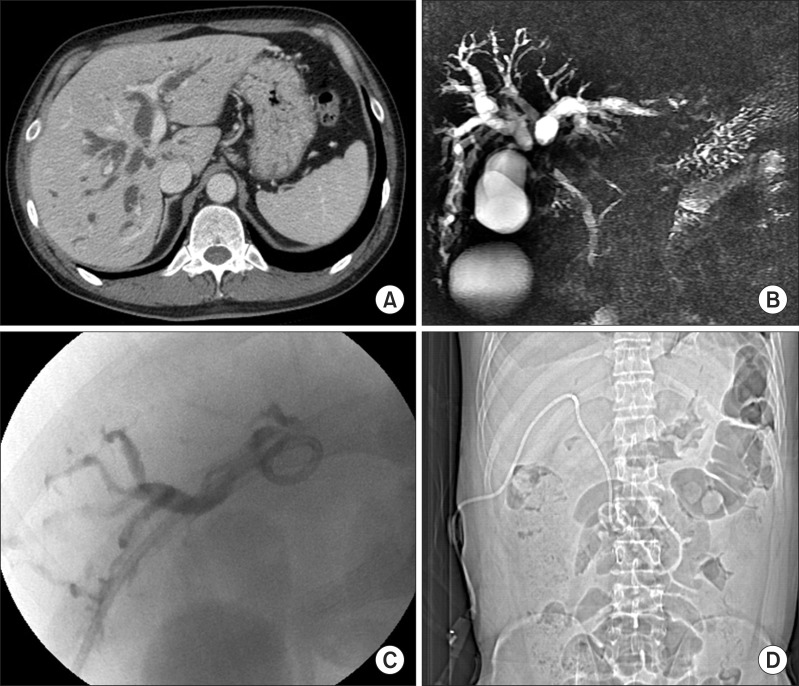
Fig. 1 Imaging finding of a patient with perihilar cholangiocarcinoma. (A) Initial computed tomography image; (B) Initial magnetic resonance cholangiography; (C) A percutaneous transhepatic biliary drainage (PTBD) tube was inserted into the right hepatic duct; (D) The PTBD tube was crossed over the hilar stenotic portion and then passed into the ampulla of Vater.
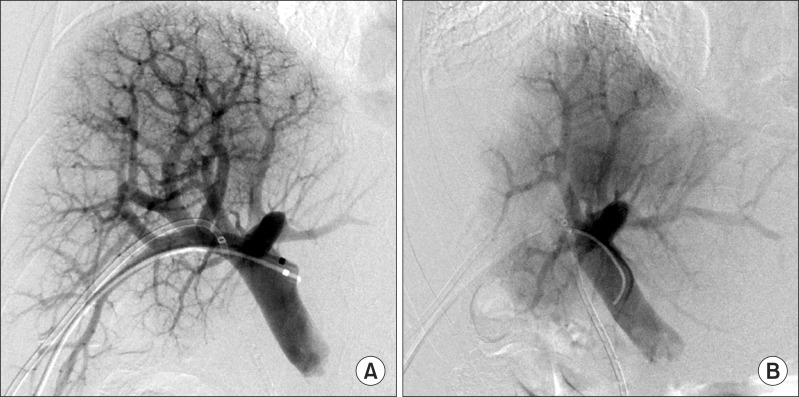
Fig. 2 Preoperative right portal vein embolization with ipsilateral approach (A) and post-embolization direct portogram (B).
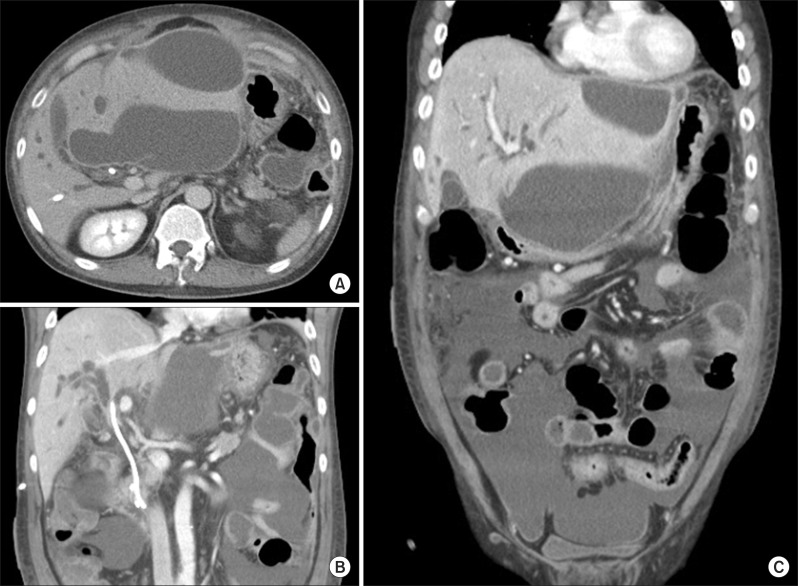
Fig. 3 Computed tomography image showing diffuse fluid collection in the abdomen and pelvis. (A) Perihepatic fluid collection; (B) A percutaneous transhepatic biliary drainage (PTBD) was placed into the right hepatic duct; (C) A large amount of fluid was collected in the pelvis.
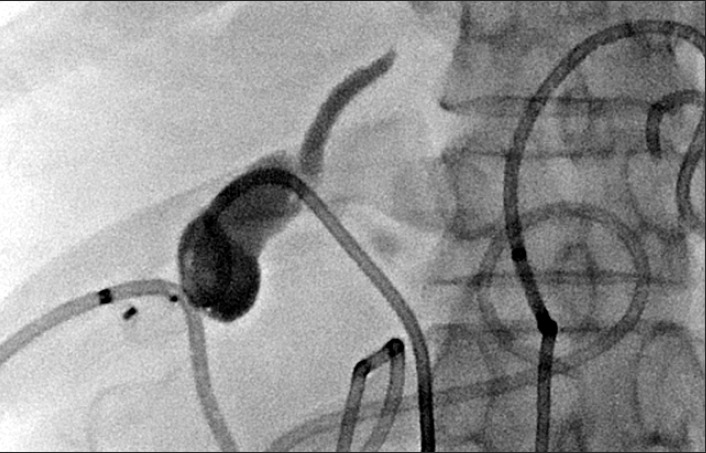
Fig. 4 Insertion of a new percutaneous transhepatic biliary drainage tube into the left hepatic duct.

Fig. 5 Embolization of the right hepatic vein and inferior right hepatic veins (arrows).
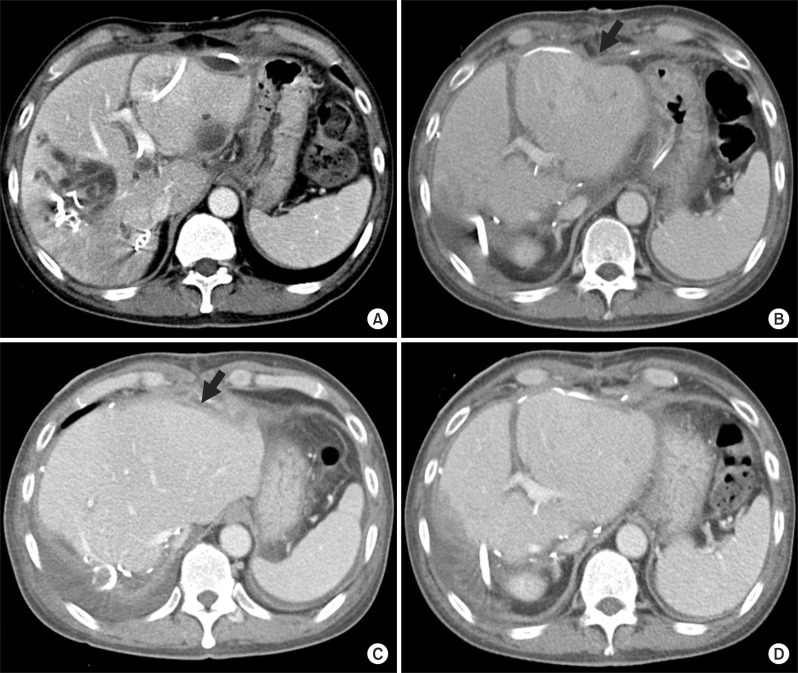
Fig. 6 Perioperative changes of computed tomography (CT) findings. (A) Liver CT taken 2 days before surgery; (B) Liver CT taken 5 days after surgery. An arrow indicates the dimpled site of liver rupture; (C) Liver CT taken 12 days after surgery. An arrow indicates the dimpled site of liver rupture; (D) Liver CT taken 12 days after surgery shows uneventful regeneration of the remnant left liver.
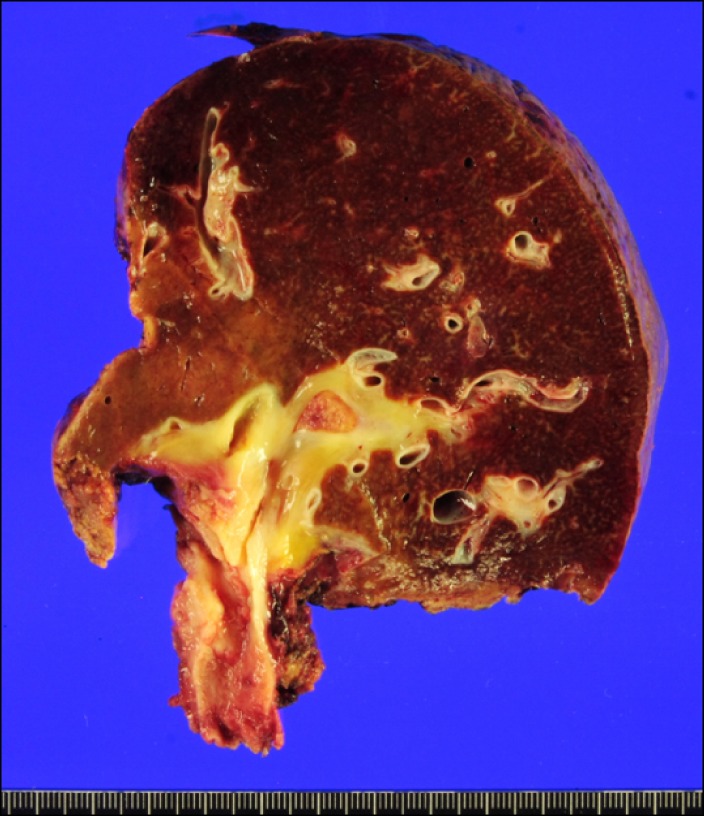
Fig. 7 Gross photograph of the resected right liver and bile duct.
Reference
-
1. Takahashi Y, Nagino M, Nishio H, et al. Percutaneous transhepatic biliary drainage catheter tract recurrence in cholangiocarcinoma. Br J Surg. 2010; 97:1860–1866. PMID: 20799295.
Article2. Maguchi H, Takahashi K, Katanuma A, et al. Preoperative biliary drainage for hilar cholangiocarcinoma. J Hepatobiliary Pancreat Surg. 2007; 14:441–446. PMID: 17909711.
Article3. Arakura N, Takayama M, Ozaki Y, et al. Efficacy of preoperative endoscopic nasobiliary drainage for hilar cholangiocarcinoma. J Hepatobiliary Pancreat Surg. 2009; 16:473–477. PMID: 19300895.
Article4. Lee SG, Lee YJ, Park KM, et al. One hundred and eleven liver resections for hilar bile duct cancer. J Hepatobiliary Pancreat Surg. 2000; 7:135–141. PMID: 10982605.
Article5. Lee SG, Song GW, Hwang S, et al. Surgical treatment of hilar cholangiocarcinoma in the new era: the Asan experience. J Hepatobiliary Pancreat Sci. 2010; 17:476–489. PMID: 19851704.
Article6. Hwang S, Song GW, Ha TY, et al. Reappraisal of percutaneous transhepatic biliary drainage tract recurrence after resection of perihilar bile duct cancer. World J Surg. 2012; 36:379–385. PMID: 22159824.
Article7. Kim TH, Lee SK, Han JH, et al. The role of endoscopic retrograde cholangiography for biliary stricture after adult living donor liver transplantation: technical aspect and outcome. Scand J Gastroenterol. 2011; 46:188–196. PMID: 20955089.
Article8. Hwang S, Lee SG, Ko GY, et al. Sequential preoperative ipsilateral hepatic vein embolization after portal vein embolization to induce further liver regeneration in patients with hepatobiliary malignancy. Ann Surg. 2009; 249:608–616. PMID: 19300228.
Article9. Hwang S. Right hepatectomy in a patient with hepatocellular carcinoma after induction of hepatic parenchymal atrophy through subsequent portal and hepatic vein embolizations. Korean J Gastroenterol. 2011; 58:162–165. PMID: 21960106.
Article10. Ko GY, Hwang S, Sung KB, et al. Interventional oncology: new options for interstitial treatments and intravascular approaches: right hepatic vein embolization after right portal vein embolization for inducing hypertrophy of the future liver remnant. J Hepatobiliary Pancreat Sci. 2010; 17:410–412. PMID: 19890603.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Right trisectionectomy with en bloc portal vein resection for perihilar cholangiocarcinoma after preoperative left portal vein stenting and sequential right portal and hepatic vein embolization
- ALPPS in a patient with periductal infiltrating intrahepatic cholangiocarcinoma
- Hilar portal vein wedge resection and patch venoplasty in patients undergoing bile duct resection for hepatobiliary malignancy: A report of two cases
- Development of perihilar cholangiocarcinoma at 29 years after first hepatectomy for hepatolithiasis
- Portal vein wedge resection and patch venoplasty using autologous and homologous vein grafts during surgery for hepatobiliary malignancies
