Synchronous Bilateral Male Breast Cancer: A Case Report
- Affiliations
-
- 1Department of Surgery, Chungbuk National University College of Medicine and Medical Research Institute, Cheongju, Korea. yjsong@chungbuk.ac.kr
- 2Department of Internal Medicine, Chungbuk National University College of Medicine and Medical Research Institute, Cheongju, Korea.
- 3Department of Pathology, Chungbuk National University College of Medicine and Medical Research Institute, Cheongju, Korea.
- KMID: 2242199
- DOI: http://doi.org/10.4048/jbc.2012.15.2.248
Abstract
- Synchronous bilateral breast cancer is extremely rare in men and has not, up to date, been reported in Korea. A 54-year-old man presented with a palpable mass in the right breast. The right nipple was retracted and bilateral axillary accessory breasts and nipples were present. On physical examination, a 2 cm-sized mass was palpated directly under the right nipple, and, with squeezing, bloody discharge developed in a single duct of the left nipple. There was no palpable mass in the left breast, and axillary lymph nodes were not palpable. Physical examination of external genitalia revealed a unilateral undescended testis on the left side. Synchronous bilateral breast cancer was diagnosed using mammography, ultrasonography, and core-needle biopsy. Histopathological examination revealed invasive ductal carcinoma in the right breast and ductal carcinoma in situ in the left breast. Bilateral total mastectomy, sentinel lymph node biopsy, and excision of accessory breasts in the axilla were performed.
Keyword
MeSH Terms
Figure
-
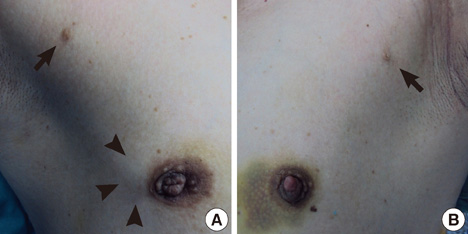
Figure 1 A mass (arrowheads) with nipple retraction was detected in the right breast. Bilateral accessory breasts in the axilla with nipples (arrows) were also present. (A) Right. (B) Left.
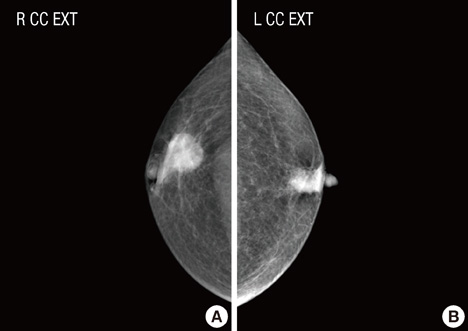
Figure 2 Mammography showed a mass in the subareolar area of both breasts. (A) Right. (B) Left.
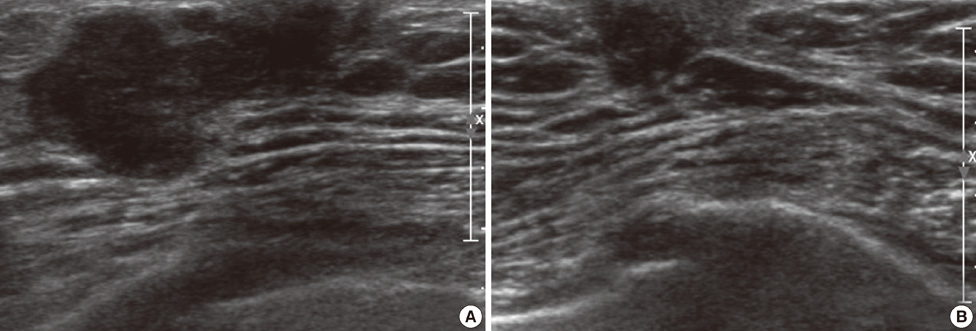
Figure 3 Ultrasonography showed a hypoechoic breast mass (BIRADS Category 5) in the subareolar area of both breasts. (A) Right. (B) Left.
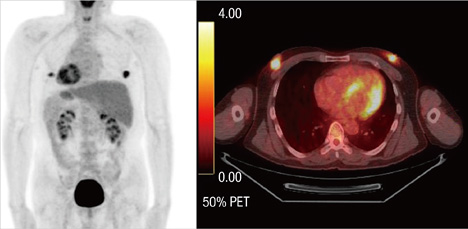
Figure 4 Positron emission tomography/computed tomography showed bilateral uptake in the subareolar area. SUVmax was 6.8 in the right breast and 5.2 in the left breast.

Figure 5 (A) The invasive ductal carcinoma in the right breast was mainly composed of micropapillary components (H&E stain, ×200). The tumor cells were suspended in a clear space. (B) The solid papillary carcinoma in the left breast showed solid tumor cell nests with focal necrosis (H&E stain, ×100).
Cited by 1 articles
-
Random Synchronous Malignancy in Male Breast: A Case Report
Manjit Sarma, Chaitanya Borde, Padma Subramanyam, Palaniswamy Shanmuga Sundaram
J Breast Cancer. 2013;16(4):442-446. doi: 10.4048/jbc.2013.16.4.442.
Reference
-
1. Weiss JR, Moysich KB, Swede H. Epidemiology of male breast cancer. Cancer Epidemiol Biomarkers Prev. 2005. 14:20–26.2. Coard K, McCartney T. Bilateral synchronous carcinoma of the male breast in a patient receiving estrogen therapy for carcinoma of the prostate: cause or coincidence? South Med J. 2004. 97:308–310.
Article3. Yaman E, Ozturk B, Coskun U, Buyukberber S, Kaya AO, Yildiz R, et al. Synchronous bilateral breast cancer in an aged male patient. Onkologie. 2010. 33:255–258.
Article4. Giordano SH. A review of the diagnosis and management of male breast cancer. Oncologist. 2005. 10:471–479.
Article5. Giordano SH, Cohen DS, Buzdar AU, Perkins G, Hortobagyi GN. Breast carcinoma in men: a population-based study. Cancer. 2004. 101:51–57.6. Lambley J, Maguire E, Yin Lam K. Synchronous bilateral breast cancer in an elderly man. Breast J. 2005. 11:153.
Article7. Cutuli B, Lacroze M, Dilhuydy JM, Velten M, De Lafontan B, Marchal C, et al. Male breast cancer: results of the treatments and prognostic factors in 397 cases. Eur J Cancer. 1995. 31A:1960–1964.
Article8. Hoque HM, Kothari A, Hamed H, Fentiman IS. Synchronous bilateral breast cancer in a patient with Klinefelter's syndrome. Int J Gen Med. 2010. 3:19–21.9. Hirose Y, Sasa M, Bando Y, Hirose T, Morimoto T, Kurokawa Y, et al. Bilateral male breast cancer with male potential hypogonadism. World J Surg Oncol. 2007. 5:60.
Article10. Qureshi K, Athwal R, Cropp G, Basit A, Adjogatse J, Bhogal RH. Bilateral synchronous ductal carcinoma in situ in a young man: case report and review of the literature. Clin Breast Cancer. 2007. 7:710–712.
Article11. Leinung S, Horn LC, Backe J. Male breast cancer: history, epidemiology, genetic and histopathology. Zentralbl Chir. 2007. 132:379–385.12. Thomas DB, Jimenez LM, McTiernan A, Rosenblatt K, Stalsberg H, Stemhagen A, et al. Breast cancer in men: risk factors with hormonal implications. Am J Epidemiol. 1992. 135:734–748.
Article13. Gómez-Pérez R, Osuna JA, Arata-Bellabarba G. Surgical vs. untreated cryptorchidism: effects on fertility. Arch Androl. 2004. 50:19–22.
Article14. Lesavoy MA, Gomez-Garcia A, Nejdl R, Yospur G, Syiau TJ, Chang P. Axillary breast tissue: clinical presentation and surgical treatment. Ann Plast Surg. 1995. 35:356–360.15. Bloom KJ, Govil H, Gattuso P, Reddy V, Francescatti D. Status of HER-2 in male and female breast carcinoma. Am J Surg. 2001. 182:389–392.
Article
