Development of Clinical Contents Model Markup Language for Electronic Health Records
- Affiliations
-
- 1R&D Center for Interoperable EHR, Seoul, Korea. april014@snu.ac.kr
- 2Department of Health Policy & Management, Seoul National University College of Medicine, Seoul, Korea.
- 3Institute of Health Policy and Management, Seoul National University Medical Research Center, Seoul, Korea.
- KMID: 2229467
- DOI: http://doi.org/10.4258/hir.2012.18.3.171
Abstract
OBJECTIVES
To develop dedicated markup language for clinical contents models (CCM) to facilitate the active use of CCM in electronic health record systems.
METHODS
Based on analysis of the structure and characteristics of CCM in the clinical domain, we designed extensible markup language (XML) based CCM markup language (CCML) schema manually.
RESULTS
CCML faithfully reflects CCM in both the syntactic and semantic aspects. As this language is based on XML, it can be expressed and processed in computer systems and can be used in a technology-neutral way.
CONCLUSIONS
CCML has the following strengths: it is machine-readable and highly human-readable, it does not require a dedicated parser, and it can be applied for existing electronic health record systems.
Keyword
Figure
-
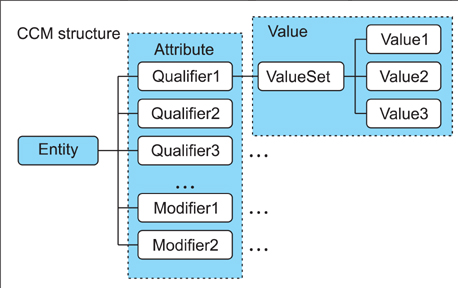
Figure 1 Clinical contents model (CCM) structure.
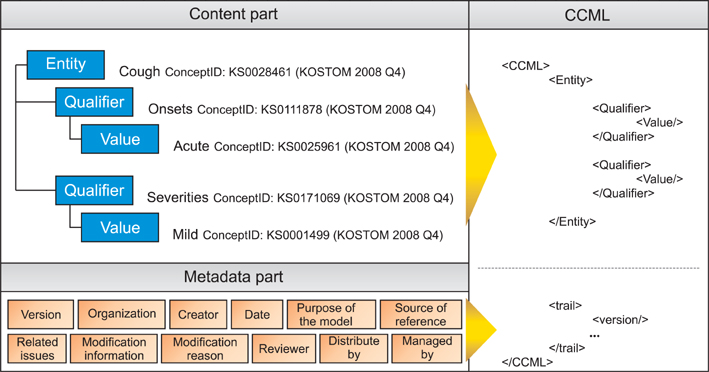
Figure 2 Overview of clinical contents model markup language (CCML) structure.
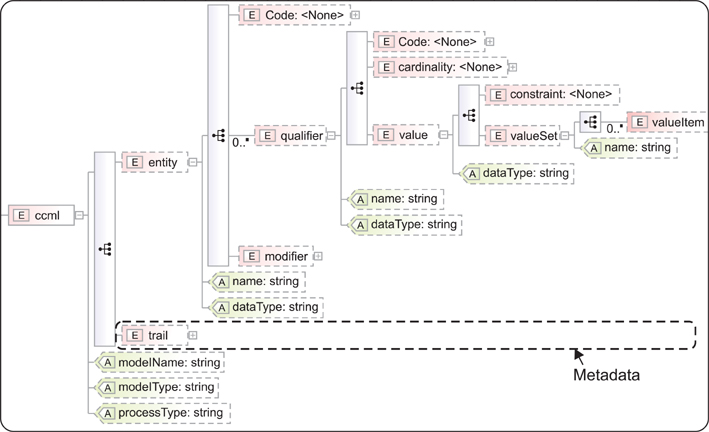
Figure 3 Overview of clinical contents model markup language (CCML) structure.
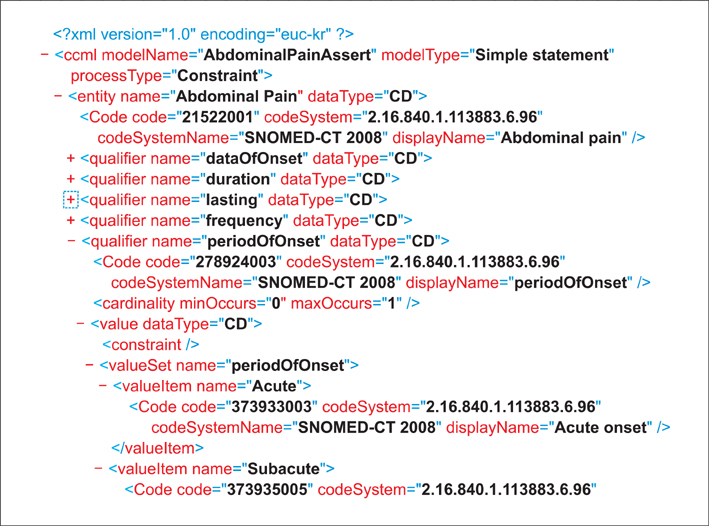
Figure 4 An example of clinical contents model markup language: the content part of model "AbdominalPainAssert".
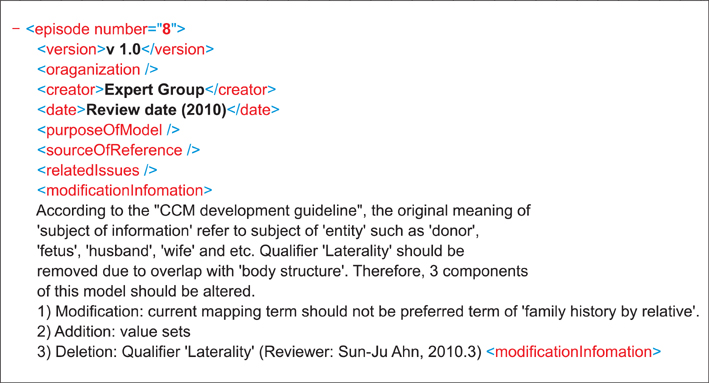
Figure 5 An example of clinical contents model markup language: the trail part of model "AbdominalPainAssert" (snippet).
Cited by 3 articles
-
Korean Anaphora Recognition System to Develop Healthcare Dialogue-Type Agent
Junggi Yang, Youngho Lee
Healthc Inform Res. 2014;20(4):272-279. doi: 10.4258/hir.2014.20.4.272.Status and Direction of Healthcare Data in Korea for Artificial Intelligence
Yu Rang Park, Soo-Yong Shin
Hanyang Med Rev. 2017;37(2):86-92. doi: 10.7599/hmr.2017.37.2.86.Mapping the Korean National Health Checkup Questionnaire to Standard Terminologies
Ji Eun Hwang, Hyeoun-Ae Park, Soo-Yong Shin
Healthc Inform Res. 2021;27(4):287-297. doi: 10.4258/hir.2021.27.4.287.
Reference
-
1. Heitmann KU, Schweiger R, Dudeck J. Discharge and referral data exchange using global standards: the SCIPHOX project in Germany. Int J Med Inform. 2003. 70(2-3):195–203.
Article2. Integrating the Healthcare Enterprise. IHE laboratory technical framework supplement 2006-2007 [Internet]. 2006. cited at 2012 Sep 15. Integrating the Healthcare Enterprise;Sharing laboratory report (XD*-LAB). Available from: http://www.ihe.net/Technical_Framework/upload/IHE_LAB_TF_Sharing_Lab_Report_XD_Lab_TI_2006_09_14.pdf.3. Health Level Seven International. Continuity of care document [Internet]. c2012. cited at 2012 Sep 1. Ann Arbor: HL7;Available from: http://www.hl7.org/documentcenter/public_temp_D458FA83-1C23-BA17-0CB3B858E7E4DC44/pressreleases/20070212.pdf.4. Braun LM, Wiesman F, van den Herik HJ, Hasman A, Korsten E. Towards patient-related information needs. Int J Med Inform. 2007. 76(2-3):246–251.
Article5. Kwak YS. Electronic health record: definition, categories and standards. J Korean Soc Med Inform. 2005. 11(1):1–15.
Article6. Haux R. Health information systems - past, present, future. Int J Med Inform. 2006. 75(3-4):268–281.
Article7. Rector AL, Nowlan WA, Kay S. Foundations for an electronic medical record. Methods Inf Med. 1991. 30(3):179–186.
Article8. Huff SM, Rocha RA, Bray BE, Warner HR, Haug PJ. An event model of medical information representation. J Am Med Inform Assoc. 1995. 2(2):116–134.
Article9. Goossen W, Goossen-Baremans A, van der Zel M. Detailed clinical models: a review. Healthc Inform Res. 2010. 16(4):201–214.
Article10. Parker CG, Rocha RA, Campbell JR, Tu SW, Huff SM. Detailed clinical models for sharable, executable guidelines. Stud Health Technol Inform. 2004. 107(Pt 1):145–148.11. Dolin RH, Alschuler L, Beebe C, Biron PV, Boyer SL, Essin D, et al. The HL7 clinical document architecture. J Am Med Inform Assoc. 2001. 8(6):552–569.
Article12. Garde S, Chen R, Leslie H, Beale T, McNicoll I, Heard S. Archetype-based knowledge management for semantic interoperability of electronic health records. Stud Health Technol Inform. 2009. 150:1007–1011.13. Goossen WT. Using detailed clinical models to bridge the gap between clinicians and HIT. Stud Health Technol Inform. 2008. 141:3–10.14. Center for Interoperable HER [Internet]. c2012. cited at 2012 Sep 1. Seoul: CiEHR;Available from: http://www.ehrkorea.org/.15. Ahn SJ, Kim Y, Yun JH, Ryu S, Cho K, Kim S, et al. Clinical contents model to ensure semantic interoperability of clinical information. J KIISE Softw Appl. 2010. 37(12):871–881.16. International Organization for Standardization. Health informatics: requirement for an electronic health record architecture. 2011. Geneva, Switzerland: International Organization for Standardization;(ISO 18308:2011).17. International Organization for Standardization. Health informatics: electronic health record-definition, scope and context. 2005. Geneva, Switzerland: International Organization for Standardization;(ISO/TR 20514:2005).18. Korea Standard Terminology of Medicine: KOSTOM [Internet]. c2012. cited at 2012 Sep 1. Seoul: Korea Health and Welfare Information Service;Available from: http://www.khwis.or.kr/.19. Ahn SJ. Development and application of development principles for clinical information model. J Korea Acad Industr Coop Soc. 2010. 11:2899–2905.
Article20. Dolin RH, Alschuler L, Boyer S, Beebe C, Behlen FM, Biron PV, et al. HL7 Clinical Document Architecture, Release 2. J Am Med Inform Assoc. 2006. 13(1):30–39.
Article21. Beeler GW. HL7 version 3: an object-oriented methodology for collaborative standards development. Int J Med Inform. 1998. 48(1-3):151–161.
Article22. Coyle JF, Mori AR, Huff SM. Standards for detailed clinical models as the basis for medical data exchange and decision support. Int J Med Inform. 2003. 69(2-3):157–174.
Article23. Kim Y, Ahn SJ, Cho KH, Ryu SH, Koh YT. Clinical contents model and structured data entry tool. 2010. Seoul: Elsevier Korea LLC;21–30.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Presentation of Structural Constraints for Discharge Note According to Clinical Document Architecture Standard
- Development Framework for HL7 Conforming Web Services
- Archetype Model-Driven Development Framework for EHR Web System
- Clinical Document Repository System for Electronic Health Record
- HL7 Development Framework based on Object-oriented Analysis & a Design for Chemotherapy Order System
