Korean J Crit Care Med.
2015 Feb;30(1):27-30. 10.4266/kjccm.2015.30.1.27.
Cardiac Rupture of the Junction of the Right Atrium and Superior Vena Cava in Blunt Thoracic Trauma
- Affiliations
-
- 1Department of Thoracic and Cardiovascular Surgery, Yonsei University Wonju College of Medicine, Wonju, Korea. mdjhoh@yonsei.ac.kr
- 2Department of Emergency Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea.
- 3Department of Anesthesiology and Pain Medicine, Yonsei University Wonju College of Medicine, Wonju, Korea.
- KMID: 2227697
- DOI: http://doi.org/10.4266/kjccm.2015.30.1.27
Abstract
- Cardiac rupture following blunt thoracic trauma is rarely encountered, since it commonly causes death at the scene. With advances in critical care, blunt cardiac rupture has been successfully treated with well-organized team approach including an emergency physician, anesthesiologist, and cardiac surgeon. We encountered a patient with blunt cardiac rupture of the junction of the superior vena cava and right atrium that extended 7 cm to the right ventricular junction. The patient was successfully resuscitated after a closed thoracostomy and pericardiocentesis with fluid loading. Cardiac injury was repaired via mid-sternotomy without cardiopulmonary bypass. The patient recovered without complications and was discharged on the 7th day after surgery.
MeSH Terms
Figure
-
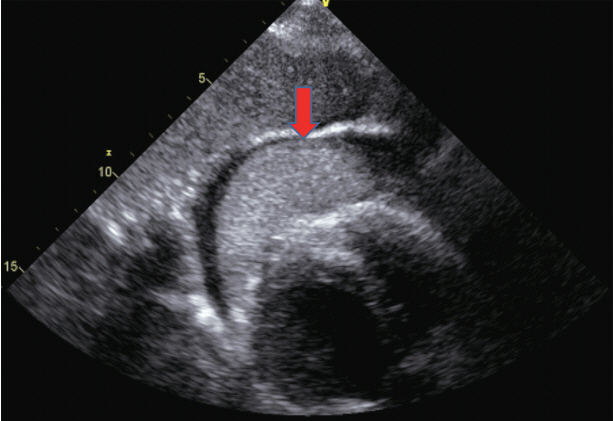
Fig. 1. The eFAST showed cardiac tamponade resulting from a large hematoma in the pericardium (red arrow). eFAST: extended focused assessment with sonography for trauma.
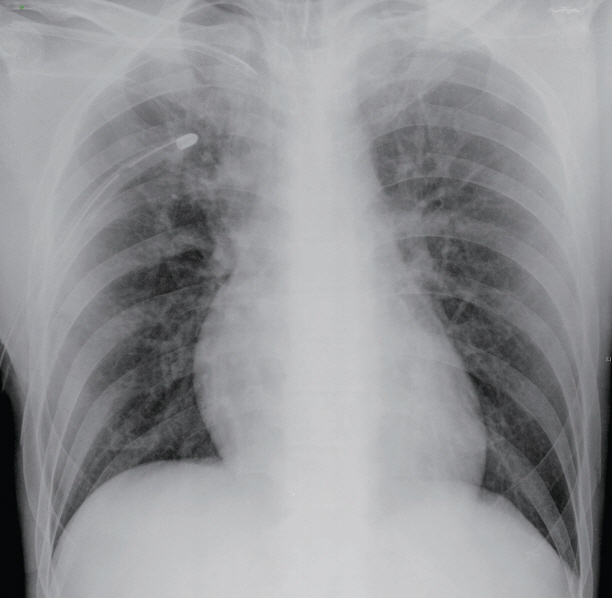
Fig. 2. Chest radiography was almost normal, except for the slightly enlarged right heart. The right chest tube was used to treat traumatic pneumothorax.

Fig. 3. Initial resuscitation with subxiphoid pericardial drainage was performed in emergency room under echocardiography.

Fig. 4. The cardiac injury included rupture of the junction of the superior vena cava and the right atrium, with a deep 7 cm laceration into right ventricular junction (black arrow).
Reference
-
References
1. Martin TD, Flynn TC, Rowlands BJ, Ward RE, Fischer RP. Blunt cardiac rupture. J Trauma. 1984; 24:287–90.
Article2. Perchinsky MJ, Long WB, Hill JG. Blunt cardiac rupture. The Emanuel Trauma Center experience. Arch Surg. 1995; 130:852–6.3. Baillot R, Dontigny L, Verdant A, Vaillancourt R, Pagé A, Pagé P, et al. Intrapericardial trauma: surgical experience. J Trauma. 1989; 29:736–40.4. Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley R. Blunt traumatic cardiac rupture. A 5-year experience. Ann Surg. 1990; 212:701–4.
Article5. Kato K, Kushimoto S, Mashiko K, Henmi H, Yamamoto Y, Otsuka T. Blunt traumatic rupture of the heart: an experience in Tokyo. J Trauma. 1994; 36:859–63.6. Malangoni MA, McHenry CR, Jacobs DG. Outcome of serious blunt cardiac injury. Surgery. 1994; 116:628–32.7. Shorr RM, Crittenden M, Indeck M, Hartunian SL, Rodriguez A. Blunt thoracic trauma. Analysis of 515 patients. Ann Surg. 1987; 206:200–5.
Article8. Elie MC. Blunt cardiac injury. Mt Sinai J Med. 2006; 73:542–52.9. Fukuoka M, Takeuchi T, Tsubota H, Mikuriya Y, Oda M, Murata S. Traumatic pericardial rupture involved with complication by blunt chest trauma. Jpn J Thorac Cardiovasc Surg. 2004; 52:423–5.
Article10. Hoffman L, Pierce D, Puumala S. Clinical predictors of injuries not identified by focused abdominal sonogram for trauma (FAST) examinations. J Emerg Med. 2009; 36:271–9.
Article11. Perchinsky MJ, Long WB, Hill JG. Blunt cardiac rupture. The Emanuel Trauma Center experience. Arch Surg. 1995; 130:852–6.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment results of cardiac tamponade due to thoracic trauma at Jeju Regional Trauma Center, Korea: a case series
- Caval Injury due to Blunt Trauma: A Report of Two cases
- Persistent Left Sperior Vena Cava Draining into the Left Atrium with Absent Right Superior Vena Cava in Tetralogy of Fallot
- A Case of Persistent Left Superior Vena Cava with Interruption of Inferior Vena Cava
- Left Atrial Rupture with Stable Vital Signs: A case report
