Delayed Rupture of Mycotic Hepatic Artery Aneurysm in a Patient with Infective Mitral Endocarditis-First Case in Korea
- Affiliations
-
- 1Department of Internal Medicine, College of Medicine, Kwandong University, Kangreung, Korea. cardio101@daum.net
- 2Department of Pediatrics, College of Medicine, Kwandong University, Kangreung, Korea.
- 3Department of General Surgery, College of Medicine, Kwandong University, Kangreung, Korea.
- 4Department of Cardiovascular Surgery, College of Medicine, Kwandong University, Kangreung, Korea.
- KMID: 2227093
- DOI: http://doi.org/10.4070/kcj.2007.37.1.43
Abstract
- Mycotic aneurysms of the hepatic artery are usually caused by mycotic infection in patients suffering with bacterial endocarditis. Mycotic aneurysms have become very rare recently due to early intensive antibiotic treatment for infective endocarditis. Despite of the non-specific symptoms, these aneurysms show a high possibility of sudden death if thye ruptured. Therefore, early detection and surgical repair of aneurysms are very important. We report here on a case of hepatic artery mycotic aneurysm that presented as sudden shock and rupture.
Keyword
MeSH Terms
Figure
-

Fig. 1 Transthoracic echocardiographic findings of the magnified mitral valve showed a mobile echogenic mass (arrow) and an attached anterior mitral leaflet (A). The transesophageal echocardiographic findings showed irregular shaped vegetation (arrow) and prolapse before mitral valve replacement (B). LA: left atrium, LV: left ventricle.

Fig. 2 Ultrasound examination showed a pulsatile hypoechoic cystic mass in the liver (A) and the Doppler scanning demonstrated arterial blood flow in this lesion (B). The white arrow indicates the cystic mass and the white arrow head indicates the mural thrombus.
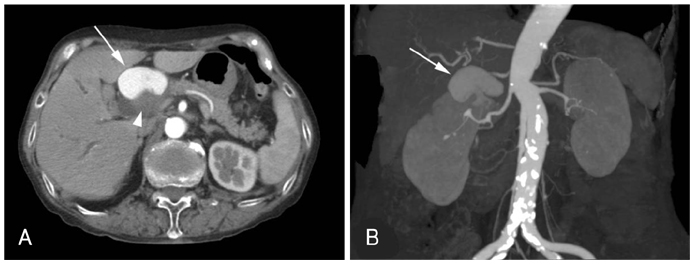
Fig. 3 Axial (A) and coronal CT scanning (B) showed a 4.4×4.1×5.2 cm sized aneurysm with a partially coagulated blood clot and strong contrast enhancement. The white arrows indicate the hepatic artery aneurysm and the arrow head indicates the mural thrombus.
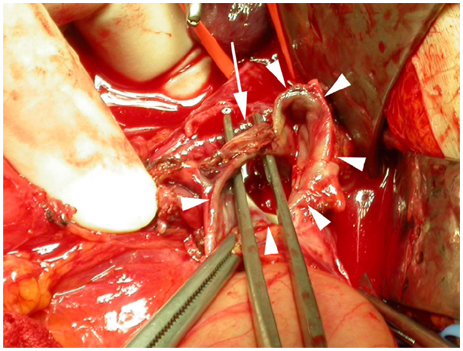
Fig. 4 The operative finding showed that aneurysm of the common hepatic artery was surgically exposed (arrow heads) and a fistula was formed from the aneurysm to the common bile duct (arrow).
Reference
-
1. Abbas MA, Fowl RJ, Stone WM, et al. Hepatic artery aneurysm: factors that predict complications. J Vasc Surg. 2003. 38:41–45.2. Porter LL 3rd, Houston MG, Kadir S. Mycotic aneurysms of the hepatic artery: treatment with arterial embolization. Am J Med. 1979. 67:697–701.3. Kim MS, Kim SH, Lee SH, et al. A case of cerebral mycotic aneurysm complicated with subarachnoid hemorrhage due to infective endocarditis. Korean Circ J. 1996. 26:1210–1217.4. Ha HG, Kim MK, Ryu JC, Kim DI, Kim DS, Hong KH. A case of infective bacterial endocarditis complicated by acute hemorrhagic pericarditis and hemoperitoneum by rupture of mycotic aneurysm at superior mesenteric artery. Korean Circ J. 1998. 28:1638–1643.5. Howling SJ, Gordon H, McArthur T, Hatfield A, Lees WR. Hepatic artery aneurysms: evaluation using three-dimensional spiral CT angiography. Clin Radiol. 1997. 52:227–230.6. Tsitouridis I, Tsinoglou K, Papastergiou C, Tsandiridis C, Stratilati S. Giant hepatic artery aneurysm as a rare cause of obstructive jaundice: Radiological evaluation. Eur J Radiol Extra. 2006. 58:9–12.7. Sechas MN, Gugulakis A, Fotiadis C, Doussaitou P. Aneurysms of visceral arteries. Chirurgie. 1997. 122:528–533.8. Cimsit B, Ozden I, Emre AS. A rare intraabdominal tumor: giant hepatic artery aneurysm. J Med Invest. 2006. 53:174–176.9. Hutchinson CE, Mackinlay JV, Buckels JA. Pseudoaneurysm of transplant hepatic artery: a late presentation. Br J Radiol. 1993. 66:158–160.10. Curran Fr, Taylor SA. Hepatic artery aneurysm. Postgrad Med J. 1986. 62:957–959.11. Lewis DR Jr, Kung H, Connon JJ. Biliary obstruction secondary to hepatic artery aneurysm: cholangiographic appearance and diagnostic considerations. Gastroenterology. 1982. 82:1446–1451.12. Harlaftis NN, Akin JT. Haemobilia from ruptured hepatic artery aneurysm: report of a case and review of the literature. Am J Surg. 1977. 133:229–232.13. Dwivedi AJ, Greben C, Krishnasastry KV. Catheter embolization of an hepatic artery aneurysm. Vasc Endovascular Surg. 2006. 40:79–83.14. Chandramohan , Khan AN, Fitzgerald S, Sherlock D, Tam E. Sonographic diagnosis and follow-up of idiopathic hepatic artery aneurysm, an unusual cause of obstructive jaundice. J Clin Ultrasound. 2001. 29:466–471.15. Katsuno A, Onda M, Tajiri T, et al. Celiac artery aneurysm: a case evaluated preoperatively with three-dimensional computed tomographic angiography. J Nippon Med Sch. 2001. 68:444–446.16. O'Driscoll D, Olliff SP, Olliff JF. Hepatic artery aneurysm. Br J Radiol. 1999. 72:1018–1025.17. Riesenman PJ, Bower TC, Oderich GS, Bjarnason H. Multiple hepatic artery aneurysms: use of transcatheter embolization for rupture. Ann Vasc Surg. 2006. 20:399–404.18. Shanlcy CJ, Shah NL, Messina LM. Common splanchnic artery aneurysms: splenic, hepatic, and celiac. Ann Vasc Surg. 1996. 10:315–322.19. Lumsden AB, Mattar SG, Allen RC, Bacha EA. Hepatic artery aneurysms: the management of 22 patients. J Surg Res. 1996. 60:345–350.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Infective Endocarditis Complicated with Multiple Myocotic Aneurysm and Mitral Valve Perforation
- A Case of Infective Endocarditis Complicated with Mycotic Aneurysm of Superior Mesenteric Artery
- A Case of Infective Bacterial Endocarditis Complicated by Acute Hemorrhagic Pericarditis and Hemoperitoneum by Rupture of Mycotic Aneurysm at Superior Mesenteric Artery
- A case of infective endocarditis complicated with asymptomatic cerebral mycotic aneurysm
- A Case of Cerebral Mycotic Aneurysm Complicated with Subarachnoid Hemorrhage due to Infective Endocarditis
