Korean J Androl.
2011 Aug;29(2):168-173. 10.5534/kja.2011.29.2.168.
Factors Causing Acute Urinary Retention after Transurethral Resection of the Prostate in Patients with Benign Prostate Hyperplasia
- Affiliations
-
- 1Department of Urology, Yeungnam University College of Medicine, Deagu, Korea. khmoon@med.yu.ac.kr
- KMID: 2226471
- DOI: http://doi.org/10.5534/kja.2011.29.2.168
Abstract
- PURPOSE
Urologists occasionally experience some cases of voiding failure after transurethral resection of prostate (TURP). Preoperative and postoperative factors attributable to acute urine retention (AUR) after catheter removal in post-TURP patients were evaluated and analyzed to determine the causative factors for AUR.
MATERIALS AND METHODS
From June 2004 to May 2008, a total of 172 patients who underwent TURP due to symptomatic benign prostatic hyperplasia (BPH) were divided into the AUR group (n=21) and the control group (n=151). The AUR group was defined as patients with voiding difficulty within 24 hours and whose residual urine volume was above 400 ml after catheter removal. The control group was defined as patients without AUR. Age, duration of symptoms, International prostate symptom score (IPSS), Quality of life score (QoL), uroflowmetry, post-void residual urine volume, preoperative serum prostate specific antigen (PSA) level, preoperative prostate volume, resected prostate volume, rate of prostate resection [resected prostate volume/preoperative prostate volume x 100], operative time and duration of catheter were retrospectively analyzed to identify which of these were the factors related with AUR after catheter removal in post-TURP patients.
RESULTS
Preoperative prostate volume was higher (90.7+/-50.4 vs 64.4+/-32.7, p=0.002) and rate of prostate resection was lower (38.8+/-8.1 vs 50.5+/-12.4, p<0.001) in AUR group compared to control group. And age, duration of symptoms, IPSS, QoL, uroflowmetry, post-void residual urine volume, preoperative serum PSA level, resected prostate volume, operative time and duration of catheter were not statistically significant in both groups. The multivariate analysis subsequently showed that preoperative prostate volume (p=0.010, OR=1.040) and rate of prostate resection (p=0.001, OR=0.901) were independent factors related with AUR after catheter removal in post-TURP patients.
CONCLUSIONS
The incidence of AUR after catheter removal was higher in post-TURP patients with high preoperative prostate volume and low rate of prostate resection. Therefore the surgeon's effort to increase the rate of prostate resection, especially in patients with large prostate volume, may lower the incidence of postoperative AUR.
MeSH Terms
Figure
-
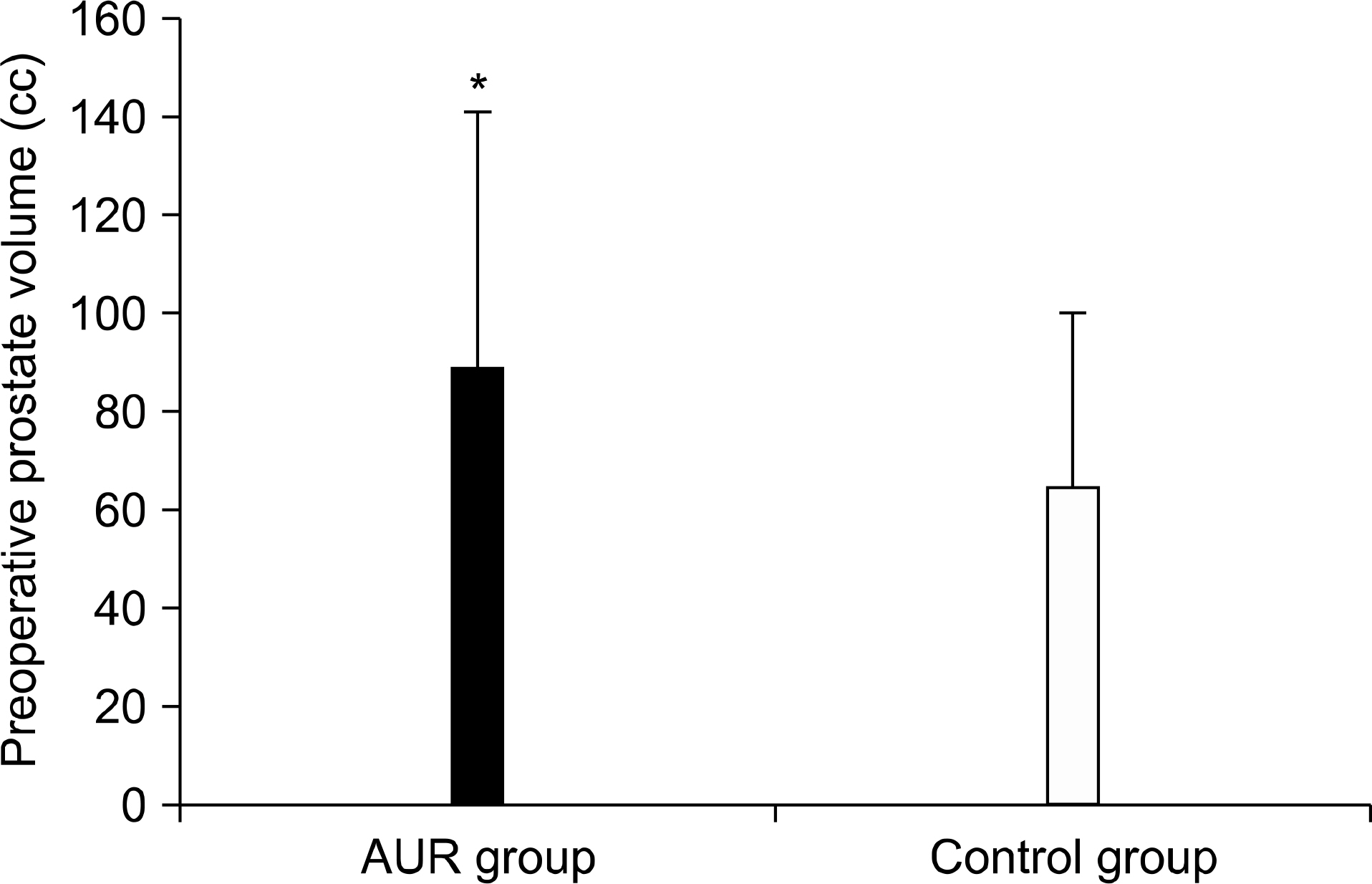
Fig. 1. Comparison of preoperative prostate volume between acute urine retention (AUR) and control group. Bars are mean±standard error of mean (∗Statistical significance was evaluated by Multiple logistic regression analysis, p<0.05).
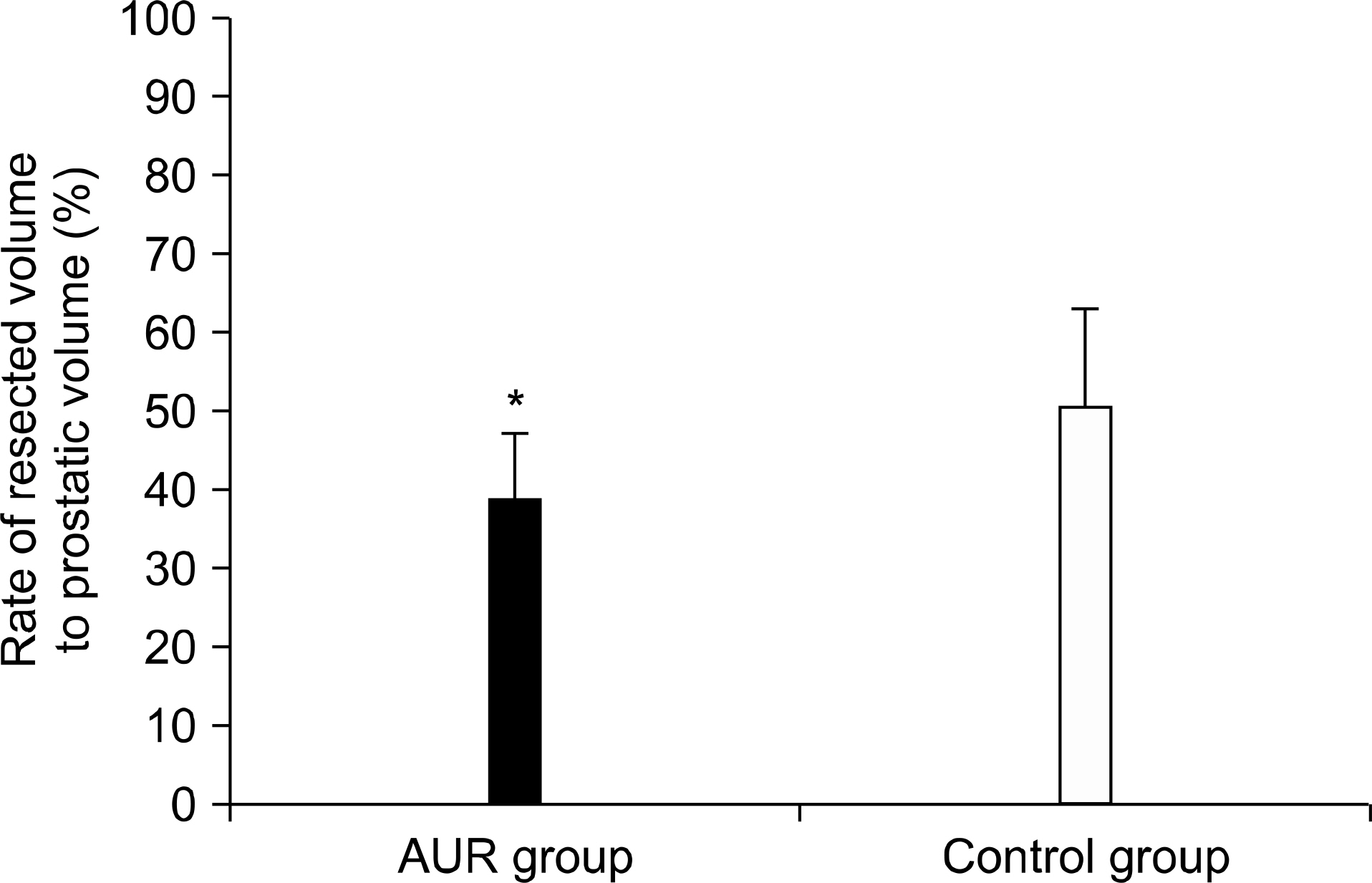
Fig. 2. Comparison of rate of resected volume to prostatic volume between acute urine retention (AUR) and control group. Bars are mean±standard error of mean (∗Statistical significance was evaluated by Multiple logistic regression analysis, p<0.05).
Reference
-
1). Han KS, Hong SJ, Chung BH. Changing trends in the management of benign prostatic hyperplasia during recent 5 years. Korean J Urol. 2005; 46:458–62.2). Kwak DY, Chang HS, Park CH, Kim CI. Longterm results of transurethral resection of the prostate for large benign prostatic hyperplasia: a comparative study with open prostatectomy. Korean J Urol. 2008; 49:31–6.
Article3). Baek M, Paick SH, Lee BK, Kang MB, Lho YS, Jung SI, et al. The efficacy of bipolar transurethral resection of the prostate in patients with large prostates(>80 g) and analysis of the postoperative results based on the resection ratio. Korean J Urol. 2008; 49:1087–93.4). Kim HG, Lee BK, Paick SH, Lho YS. Efficacy of bipolar transurethral resection of the prostate: comparison with standard monopolar transurethral resection of the prostate. Korean J Urol. 2006; 47:377–80.
Article5). Hakenberg OW, Helke C, Manseck A, Wirth MP. Is there a relationship between the amount of tissue removed at transurethral resection of the prostate and clinical improvement in benign prostatic hyperplasia. Eur Urol. 2001; 39:412–7.
Article6). Rassweiler J, Teber D, Kuntz R, Hofmann R. Complications of transurethral resection of the prostate (TURP)–incidence, management, and prevention. Eur Urol. 2006; 50:969–79.
Article7). Bishop P. Bipolar transurethral resection of the prostate–a new approach. AORN J. 2003; 77:979–83.
Article8). Reich O, Gratzke C, Bachmann A, Seitz M, Schlenker B, Hermanek P, et al. Urology Section of the Bavarian Working Group for Quality Assurance. Morbidity, mortality and early outcome of transurethral resection of the prostate: a prospective multicenter evaluation of 10,654 patients. J Urol. 2008; 180:246–9.
Article9). Lim KB, Wong MY, Foo KT. Transurethral resection of prostate (TURP) through the decades–a comparison of results over the last thirty years in a single institution in Asia. Ann Acad Med Singapore. 2004; 33:775–9.10). Starkman JS, Santucci RA. Comparison of bipolar transurethral resection of the prostate with standard transurethral prostatectomy: shorter stay, earlier catheter removal and fewer complications. BJU Int. 2005; 95:69–71.
Article11). Oh CS, Choi KY, Park RJ. Relationship between the amount of tissue removed at transurethral resection of the prostate and clinical improvement in benign prostate hyperplasia. Korean J Urol. 2003; 44:866–70.12). Aagaard J, Jonler M, Fuglsig S, Christensen LL, Jorgensen HS, Norgaard JP. Total transurethral resection versus minimal transurethral resection of the prostate–a 10-year follow-up study of urinary symptoms, uroflowmetry and residual volume. Br J Urol. 1994; 74:333–6.13). Chen SS, Hong JG, Hsiao YJ, Chang LS. The correlation between clinical outcome and residual prostatic weight ratio after transurethral resection of the prostate for benign prostatic hyperplasia. BJU Int. 2000; 85:79–82.
Article14). Chang HS, Park CH, Kim CI. Transitional zone volume: a predictor of acute urinary retention in patients with benign prostatic hyperplasia. Korean J Urol. 2005; 46:259–63.15). Jacobsen SJ, Jacobson DJ, Girman CJ, Roberts RO, Rhodes T, Guess HA, et al. Natural history of prostatism: risk factors for acute urinary retention. J Urol. 1997; 158:481–7.
Article16). Wein AJ. Lower urinary tract dysfunction in neurologic injury and disease. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Campbell's urology. 9th ed.Philadelphia: Saunders;2007. p. 2040–1.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Transurethral Resection of Prostate under Local Anesthesia in Patients with Benign Prostatic Hyperplasia
- Fluid extravasation caused by bladder perforation during bipolar transurethral resection using saline solution: a case report
- Clinical Observation on Transurethral Resection of Prostate and Suprapubic Prostatectomy for Benign Prostatic Hypertrophy
- Transurethral Needle Ablation of BPH
- Prostate Metastasis of Renal Cell Carcinoma
