Angioplasty for Difficult Complex Lesions With Using the Venture(TM) Catheter for Wire Placement
- Affiliations
-
- 1Department of Internal Medicine, Pusan National University School of Medicine, Busan, Korea. aangell@hananet.net
- 2Department of Thoracic and Cardiovascular Surgery, Pusan National University School of Medicine, Busan, Korea.
- KMID: 2225792
- DOI: http://doi.org/10.4070/kcj.2008.38.5.287
Abstract
- We report here on the use of the Venture(TM) catheter to facilitate successful advancement of a guidewire across difficult, complex lesions after the prior attempts at guide wire passage were unsuccessful with using standard wires. This Venture(TM) catheter may increase the success rate and reduce the procedural time for such a challenging interventional procedure.
Keyword
MeSH Terms
Figure
-
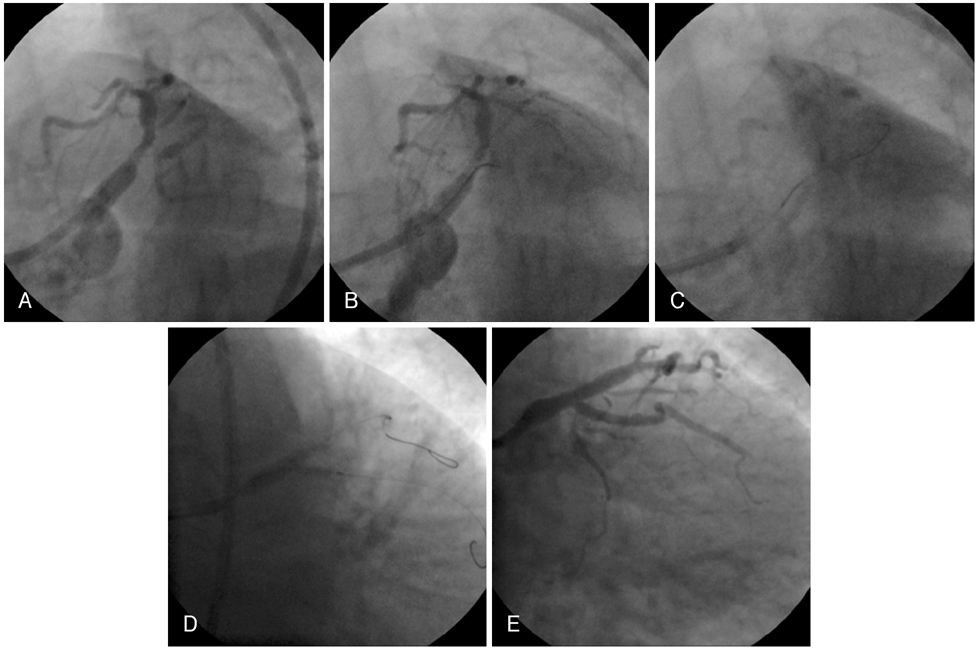
Fig. 1 Angiographic findings of first case. A: subtotal occlusion without a visible stump at the ostium of the circumflex artery and there is tubular eccentric luminal narrowing at the ostium of the left anterior descending artery. B: the tip of the Venture Catheter was deflected and engaged at the ostium of the circumflex artery. C: a guidewire is advanced into the distal vessel. D: kissing ballooning after crushing at the bifurcation lesion. E: the final angiographic result following balloon dilation and placement of two drug-eluting stents.
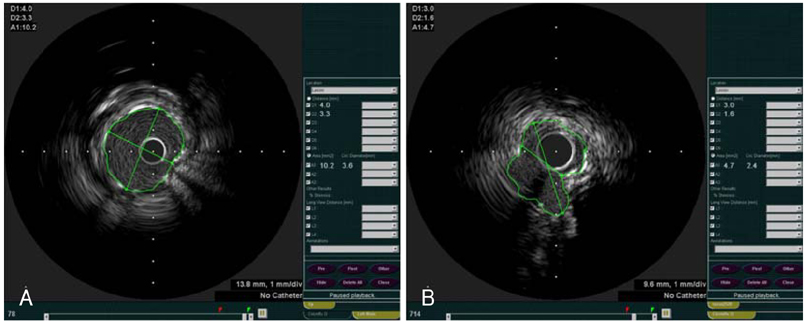
Fig. 2 IVUS findings of first case. A: post-procedural IVUS findings of the left main artery (minimal stent area: 10.2 mm2). B: post-procedural IVUS findings of the circumflex artery ostium (minimal stent area: 4.7 mm2). IVUS: intravascular ultrasound.

Fig. 3 Angiographic findings of second case. A: initial coronary angiography showed the diffusely diseased lumen of the left anterior descending artery. B: a severely angulated and subocclusive lesion at the ostium of the circumflex artery. C: an unsuccessful attempt to pass a guidewire in the ostium of the circumflex artery by using a microcatheter. This was successfully advanced into the proximal lesion, but it was unable to cross the second angle of the lesion. D: the Venture Catheter in a curved configuration engaging the circumflex stump and the guidewire was advanced into the distal vessel. E: kissing ballooning after crushing at the bifurcation lesion. F, G: final results.
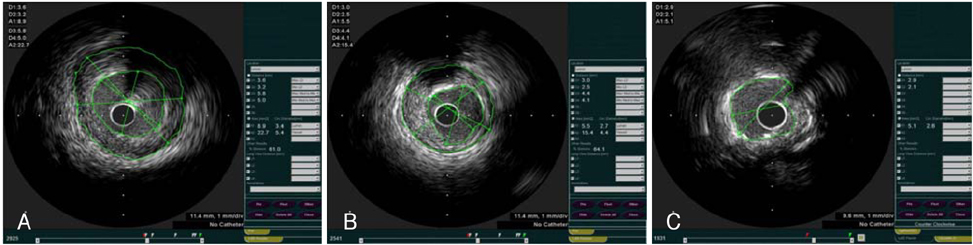
Fig. 4 IVUS findings of second case. A: pre-procedural IVUS findings of the distal left main artery (the cross sectional area is 8.9 mm2 and there is a 61% plaque burden). B: pre-procedural IVUS findings of the left anterior descending artery ostium (the cross sectional area is 5.5 mm2 and there is a 64% plaque burden). C: post-procedural IVUS findings of the circumflex artery ostium (minimal stent area: 5.1 mm2). IVUS: intravascular ultrasound.
Reference
-
1. Ellis SG, Vandormael MG, Cowley MJ, et al. Coronary morphologic and clinical determinants of procedural outcome with angioplasty for multivessel coronary disease: implications for patient selection. Circulation. 1990. 82:1193–1202.2. Tan K, Sulke N, Taub N, Sowton E. Clinical and lesion morphologic determinants of coronary angioplasty success and complications: current experience. J Am Coll Cardiol. 1995. 25:855–865.3. Yum JH, Jeong MH, Seoung KB, et al. Percutaneous coronary intervention using crosswireNT in total occlusion of coronary artery. Korean Circ J. 2002. 32:125–130.4. Naidu SS, Wong SC. Novel intracoronary steerable support catheter for complex coronary intervention. J Invasive Cardiol. 2006. 18:80–81.5. McClure SJ, Wahr DW, Webb JG. Venture wire control catheter. Catheter Cardiovasc Interv. 2005. 66:346–350.6. Aranzulla TC, Colombo A, Sangiorgi GM. Successful endovascular renal artery aneurysm exclusion using the Venture™ Catheter and covered stent implantation: a case report and review of the literature. J Invasive Cardiol. 2007. 19:E246–E253.7. McNulty E, Cohen J, Chou T, Shunk K. A "grapple hook" technique using deflectable tip catheter to facilitate complex proximal circumflex interventions. Catheter Cardiovasc Interv. 2006. 67:46–48.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Broken Guidewire Fragment in the Radio-brachial Artery During Transradial Sheath Placement: Percutaneous Retrieval via Femoral Approach
- Endovascular interventions for central vein stenosis
- Two Cases of Coronary Pseudo-Lesion Induced in the Left Circumflex Artery and the Right Coronary Artery by the Angioplasty Guide-Wire
- Coronary Angioplasty for the Total Occlusion Using a New Hydrophilic Guidewire, Crosswire (TM)
- Novel Wire-Guided Scalpel to Facilitate Central Venous Catheter Insertion without a Skin Bridge
