Stenting of the Left Main Coronary Artery in a Patient With Takayasu's Arteritis
- Affiliations
-
- 1Department of Internal Medicine, Vision 21 Cardiac and Vascular Center, Inje University, Ilsan Paik Hospital, Goyang, Korea. medngj@gmail.com
- KMID: 2225152
- DOI: http://doi.org/10.4070/kcj.2011.41.1.34
Abstract
- Management of Takayasu's arteritis of the left main coronary artery (LMCA) is difficult because of the possibility of restenosis. Clinically significant stenotic lesions must be considered anatomical correlation. Many studies have reported that the management of stenotic lesions of the LMCA with endoluminal stenting and balloon angioplasty and de-novo stenting is safe and effective for patients with Takayasu's arteritis. We report the case of a patient with Takayasu's arteritis of the LMCA. The patient had undergone two consecutive percutaneous coronary interventions because of recurrent restenosis of in-stent lesions, and eventually underwent coronary artery bypass graft (CABG) surgery for myocardial infarction in the same lesion. We suggested treatment with CABG because the pathophysiology of Takayasu's arteritis is different from that of atherosclerotic stenosis.
MeSH Terms
Figure
-
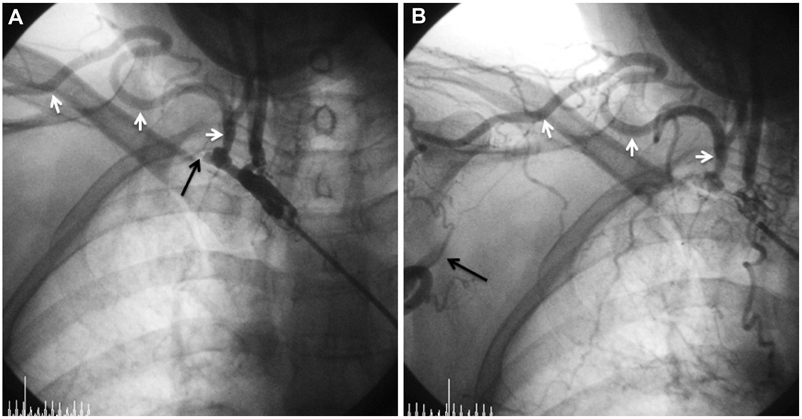
Fig. 1 Angiography of the right subclavian artery show total occlusion (black arrow) near the origin and marked dilation of the collateral artery (white arrows) originating from the thyrocervical trunk in the early phase (A) and a reconstituted axillary artery (black arrow) via dilated collaterals (white arrow) in later phase (B).
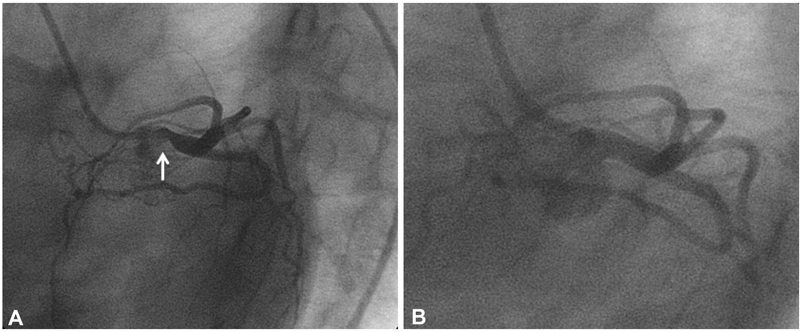
Fig. 2 Angiography of the left coronary angiography show focal stenosis in the ostium of left main coronary artery (A) and a paclitaxel-eluting stent deployed in the ostium of the left main coronary artery (B).
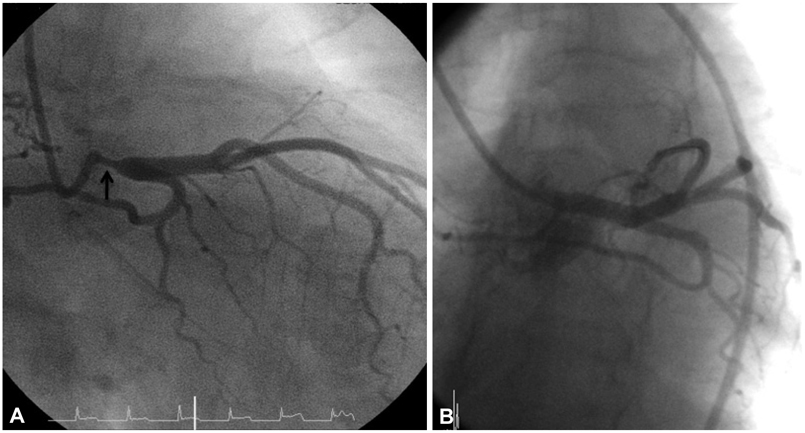
Fig. 3 A follow-up coronary angiography shows 75% segmental stenosis in the proximal portion of the in-stent lesion area (A) and another paclitaxel-eluting stent (TAXUS™) deployed in the in-stent lesion (B).

Fig. 4 Coronary angiography shows tight insent restenosis after second intervention in the ostium of the left main coronary artery.
Reference
-
1. Lupi-Herrera E, Sánchez-Torres G, Marcushamer J, Mispireta J, Horwitz S, Vela JE. Takayasu arteritis: clinical study of 107 cases. Am Heart J. 1977. 93:94–103.2. Hall S, Barr W, Lie JT, Stanson AW, Kazmier FJ, Hunder GG. Takayasu arteritis: a study of 32 North America patients. Medicine. 1985. 64:89–99.3. Bulut S, Al Hashimin HM, Verheugt FW. Left main stem disease in a patient with Takayasu's arteritis. Neth Heart J. 2007. 15:260–262.4. Endo M, Tomizawa Y, Nishida H, et al. Angiographic findings and surgical treatments of coronary artery involvement in Takayasu arteritis. J Thorac Cardiovasc Surg. 2003. 125:570–577.5. Furukawa Y, Tamura T, Toma M, et al. Sirolimus-eluting stent for in-stent restenosis of left main coronary artery in Takayasu arteritis. Circ J. 2005. 69:752–755.6. Son JW, Koh KK, Dang Q, Choi IS, Shin EK. Recurrent restenosis following stent and rotational atherectomy of coronary artery stenosis in Takayasu's arteritis. Int J Cardiol. 1998. 65:295–300.7. Kang WC, Han SH, Ahn TH, Shin EK. Successful management of left main coronary artery stenosis with a paclitaxel-eluting stent in Takayasu's arteritis. Int J Cardiol. 2006. 108:120–123.8. Sakai H, Oyama H, Kishimoto N, Takahashi M, Urasawa K, Tsutsui H. Revascularization of malignant coronary instent restenosis resulting from Takayasu's arteritis using sirolimus-eluting stent. Int Heart J. 2006. 47:795–801.9. Amir O, Kar B, Civitello AB, Palanichamy N, Shakir A, Delgado RM 3rd. Unprotected left main stent placement in a patient with Takayasu's arteritis. Tex Heart Inst J. 2006. 33:253–255.10. Kim KC, Park JI, Lee J, et al. Clinical characteristics of Takayasu's arteritis. Korean Circ J. 2001. 31:1106–1116.11. Matsubara O, Kuwata T, Nemoto T, Kasuga T, Numano F. Coronary artery lesions in Takayasu's arteritis. Heart Vessels Suppl. 1992. 7:26–31.12. Park JH, Han MC, Kim SH, Oh BH, Park YB, Seo JD. Takayasu arteritis: angiographic findings and results of angioplasty. AJR Am J Roentgenol. 1989. 153:1069–1074.13. Trazzera S, Colasacco J, Ong L. Takayasu arteritis with unstable angina and aortic insufficiency. Am Heart J. 1995. 130:1122–1124.14. Antelmi I, Magalhães L, Caramelli B, et al. Salvage coronary angioplasty in a young patient with Takayasu arteritis and myocardial infarction. Arq Bras Cardiol. 1993. 60:37–38.15. Kang KT, Jeong MH, Jeong WK, et al. Long-term clinical follow-up in a case of Takayasu's arteritis involving the ostium of left coronary artery after ostioplasty. Korean Circ J. 2001. 31:246–250.16. Punamiya K, Bates ER, Shea MJ, Muller DW. Endoluminal stenting for unprotected left main stenosis in Takayasu's arteritis. Cathet Cardiovasc Diagn. 1997. 40:272–275.17. Kang WC, Han SH, Oh KJ, Ahn TH, Shin EK. Implantation of a drug-eluting for the coronary artery stenosis of Takayasu arteritis: de novo and in-stent restenosis. Circulation. 2006. 113:e735–e737.18. Park JS, Lee HC, Lee SK, et al. Takayasu's arteritis involving the ostia of three large coronary arteries. Korean Circ J. 2009. 39:551–555.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Takayasu's Arteritis Associated with Aortic Regurgitation and Coronary Artery Involvement
- Percutaneous transluminal coronary angioplasty for ostial stenosis of the left coronary artery
- A Case of Takayasu's Arteritis Presented by Stenosis of Main Pulmonary Artery and Obstruction of the Right Coronary Artery
- A Case of Left Main Coronary Artery Disease Treated with Medication
- Takayasu's Arteritis Associated with Coronary and Renal Arteries Stenosis
